| The urinary organs comprise the kidneys, which secrete the urine, the ureters, or ducts, which convey urine to the urinary bladder, where it is for a time retained; and the urethra, through which it is discharged from the body. | 1 |
| |
| 1. The Kidneys (Renes)—The kidneys are situated in the posterior part of the abdomen, one on either side of the vertebral column, behind the peritoneum, and surrounded by a mass of fat and loose areolar tissue. Their upper extremities are on a level with the upper border of the twelfth thoracic vertebra, their lower extremities on a level with the third lumbar. The right kidney is usually slightly lower than the left, probably on account of the vicinity of the liver. The long axis of each kidney is directed downward and lateralward; the transverse axis backward and lateralward. | 2 |
| Each kidney is about 11.25 cm. in length, 5 to 7.5 cm. in breadth, and rather more than 2.5 cm. in thickness. The left is somewhat longer, and narrower, than the right. The weight of the kidney in the adult male varies from 125 to 170 gm., in the adult female from 115 to 155 gm. The combined weight of the two kidneys in proportion to that of the body is about 1 to 240. | 3 |
| The kidney has a characteristic form, and presents for examination two surfaces, two borders, and an upper and lower extremity. | 4 |
| |
| Relations.—The anterior surface (facies anterior) (Figs. 1120 and 1122) of each kidney is convex, and looks forward and lateralward. Its relations to adjacent viscera differ so completely on the two sides that separate descriptions are necessary. | 5 |
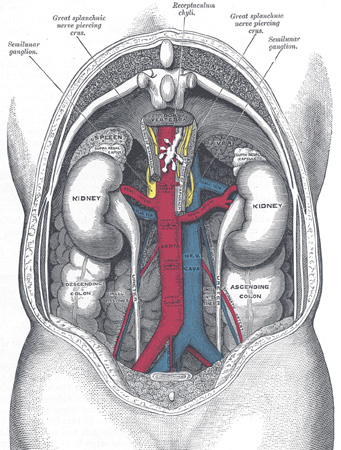 |
FIG. 1120– The relations of the viscera and large vessels of the abdomen. (Seen from behind, the last thoracic vertebra being well raised.) (See enlarged image) |
| |
| |
| Anterior Surface of Right Kidney.—A narrow portion at the upper extremity is in relation with the right suprarenal gland. A large area just below this and involving about three-fourths of the surface, lies in the renal impression on the inferior surface of the liver, and a narrow but somewhat variable area near the medial border is in contact with the descending part of the duodenum. The lower part of the anterior surface is in contact laterally with the right colic flexure, and medially, as a rule, with the small intestine. The areas in relation with the liver and small intestine are covered by peritoneum; the suprarenal, duodenal, and colic areas are devoid of peritoneum. | 6 |
| |
| Anterior Surface of Left Kidney.—A small area along the upper part of the medial border is in relation with the left suprarenal gland, and close to the lateral border is a long strip in contact with the renal impression on the spleen. A somewhat quadrilateral field, about the middle of the anterior surface, marks the site of contact with the body of the pancreas, on the deep surface of which are the lienal vessels. Above this is a small triangular portion, between the suprarenal and splenic areas, in contact with the postero-inferior surface of the stomach. Below the pancreatic area the lateral part is in relation with the left colic flexure, the medial with the small intestine. The areas in contact with the stomach and spleen are covered by the peritoneum of the omental bursa, while that in relation to the small intestine is covered by the peritoneum of the general cavity; behind the latter are some branches of the left colic vessels. The suprarenal, pancreatic, and colic areas are devoid of peritoneum. | 7 |
 |
FIG. 1121– Posterior abdominal wall, after removal of the peritoneum, showing kidneys, suprarenal capsules, and great vessels. (Corning). (See enlarged image) |
| |
| The Posterior Surface (facies posterior) (Figs. 1123, 1124).—The posterior surface of each kidney is directed backward and medialward. It is imbedded in areolar and fatty tissue and entirely devoid of peritoneal covering. It lies upon the diaphragm, the medial and lateral lumbocostal arches, the Psoas major, the Quadratus lumborum, and the tendon of the Transversus abdominis, the subcostal, and one or two of the upper lumbar arteries, and the last thoracic, iliohypogastric, and ilioinguinal nerves. The right kidney rests upon the twelfth rib, the left usually on the eleventh and twelfth. The diaphragm separates the kidney from the pleura, which dips down to form the phrenicocostal sinus, but frequently the muscular fibers of the diaphragm are defective or absent over a triangular area immediately above the lateral lumbocostal arch, and when this is the case the perinephric areolar tissue is in contact with the diaphragmatic pleura. | 8 |
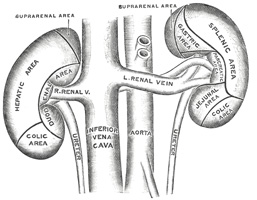 |
FIG. 1122– The anterior surfaces of the kidneys, showing the areas of contact of neighboring viscera. (See enlarged image) |
| |
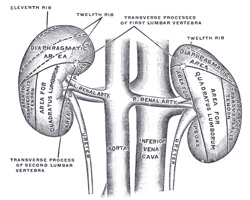 |
FIG. 1123– The posterior surfaces of the kidneys, showing areas of relation to the parietes. (See enlarged image) |
| |
| |
| Borders.—The lateral border (margo lateralis; external border) is convex, and is directed toward the postero-lateral wall of the abdomen. On the left side it is in contact at its upper part, with the spleen. | 9 |
| The medial border (margo medialis; internal border) is concave in the center and convex toward either extremity; it is directed forward and a little downward. Its central part presents a deep longitudinal fissure, bounded by prominent overhanging anterior and posterior lips. This fissure is named the hilum, and transmits the vessels, nerves, and ureter. Above the hilum the medial border is in relation with the suprarenal gland; below the hilum, with the ureter. | 10 |
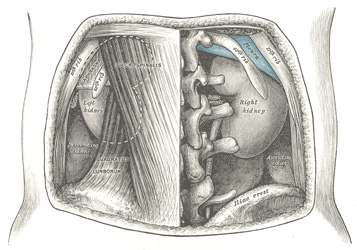 |
FIG. 1124– The relations of the kidneys from behind. (See enlarged image) |
| |
| |
| Extremities.—The superior extremity (extremitas superior) is thick and rounded, and is nearer the median line than the lower; it is surmounted by the suprarenal gland, which covers also a small portion of the anterior surface. | 11 |
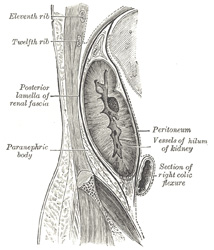 |
FIG. 1125– Sagittal section through posterior abdominal wall, showing the relations of the capsule of the kidney. (After Gerota). (See enlarged image) |
| |
| The inferior extremity (extremitas inferior) is smaller and thinner than the superior and farther from the median line. It extends to within 5 cm. of the iliac crest. | 12 |
| The relative position of the main structures in the hilum is as follows: the vein is in front, the artery in the middle, and the ureter behind and directed downward. Frequently, however, branches of both artery and vein are placed behind the ureter. | 13 |
| |
| Fixation of the Kidney (Figs. 1125, 1126).—The kidney and its vessels are imbedded in a mass of fatty tissue, termed the adipose capsule, which is thickest at the margins of the kidney and is prolonged through the hilum into the renal sinus. The kidney and the adipose capsule are enclosed in a sheath of fibrous tissue continuous with the subperitoneal fascia, and named the renal fascia. At the lateral border of the kidney the renal fascia splits into an anterior and a posterior layer. The anterior layer is carried medialward in front of the kidney and its vessels, and is continuous over the aorta with the corresponding layer of the opposite side. The posterior layer extends medialward behind the kidney and blends with the fascia on the Quadratus lumborum and Psoas major, and through this fascia is attached to the vertebral column. Above the suprarenal gland the two layers of the renal fascia fuse, and unite with the fascia of the diaphragm; below they remain separate, and are gradually lost in the subperitoneal fascia of the iliac fossa. The renal fascia is connected to the fibrous tunic of the kidney by numerous trabeculæ, which traverse the adipose capsule, and are strongest near the lower end of the organ. Behind the fascia renalis is a considerable quantity of fat, which constitutes the paranephric body. The kidney is held in position partly through the attachment of the renal fascia and partly by the apposition of the neighboring viscera. | 14 |
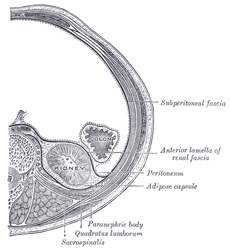 |
FIG. 1126– Transverse section, showing the relations of the capsule of the kidney. (After Gerota.) (See enlarged image) |
| |
| |
| General Structure of the Kidney.—The kidney is invested by a fibrous tunic, which forms a firm, smooth covering to the organ. The tunic can be easily stripped off, but in doing so numerous fine processes of connective tissue and small bloodvessels are torn through. Beneath this coat a thin, wide-meshed net-work of unstriped muscular fiber forms an incomplete covering to the organ. When the capsule is stripped off, the surface of the kidney is found to be smooth and even and of a deep red color. In infants fissures extending for some depth may be seen on the surface of the organ, a remnant of the lobular construction of the gland. The kidney is dense in texture, but is easily lacerable by mechanical force. If a vertical section of the kidney be made from its convex to its concave border, it will be seen that the hilum expands into a central cavity, the renal sinus, this contains the upper part of the renal pelvis and the calyces, surrounded by some fat in which are imbedded the branches of the renal vessels and nerves. The renal sinus is lined by a prolongation of the fibrous tunic, which is continued around the lips of the hilum. The renal calyces, from seven to thirteen in number, are cup-shaped tubes, each of which embraces one or more of the renal papillæ; they unite to form two or three short tubes, and these in turn join to form a funnel-shaped sac, the renal pelvis. The renal pelvis, wide above and narrow below where it joins the ureter, is partly outside the renal sinus. The renal calyces and pelvis form the upper expanded end of the excretory duct of the kidney. | 15 |
| The kidney is composed of an internal medullary and an external cortical substance. | 16 |
| The medullary substance (substantia medullaris) consists of a series of red-colored striated conical masses, termed the renal pyramids, the bases of which are directed toward the circumference of the kidney, while their apices converge toward the renal sinus, where they form prominent papillæ projecting into the interior of the calyces. | 17 |
| The cortical substance (substantia corticalis) is reddish brown in color and soft and granular in consistence. It lies immediately beneath the fibrous tunic, arches over the bases of the pyramids, and dips in between adjacent pyramids toward the renal sinus. The parts dipping in between the pyramids are named the renal columns (Bertini), while the portions which connect the renal columns to each other and intervene between the bases of the pyramids and the fibrous tunic are called the cortical arches (indicated between A and A’ in Fig. 1127). If the cortex be examined with a lens, it will be seen to consist of a series of lighter-colored, conical areas, termed the radiate part, and a darker-colored intervening substance, which from the complexity of its structure is named the convoluted part. The rays gradually taper toward the circumference of the kidney, and consist of a series of outward prolongations from the base of each renal pyramid. | 18 |
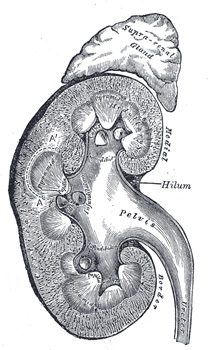 |
FIG. 1127– Vertical section of kidney. (See enlarged image) |
| |
| |
| Minute Anatomy.—The renal tubules (Fig. 1028), of which the kidney is for the most part made up, commence in the cortical substance, and after pursuing a very circuitous course through the cortical and medullary substances, finally end at the apices of the renal pyramids by open mouths, so that the fluid which they contain is emptied, through the calyces, into the pelvis of the kidney. If the surface of one of the papillæ be examined with a lens, it will be seen to be studded over with minute openings, the orifices of the renal tubules, from sixteen to twenty in number, and if pressure be made on a fresh kidney, urine will be seen to exude from these orifices. The tubules commence in the convoluted part and renal columns as the renal corpuscles, which are small rounded masses of a deep red color, varying in size, but of an average of about 0.2 mm. in diameter. Each of these little bodies is composed of two parts: a central glomerulus of vessels, and a membranous envelope, the glomerular capsule (capsule of Bowman), which is the small pouch-like commencement of a renal tubule. | 19 |
| The glomerulus is a lobulated net-work of convoluted capillary bloodvessels, held together by scanty connective tissue. This capillary net-work is derived from a small arterial twig, the afferent vessel, which enters the capsule, generally at a point opposite to that at which the latter is connected with the tubule; and the resulting vein, the efferent vessel, emerges from the capsule at the same point. The afferent vessel is usually the larger of the two (Fig. 1129). The glomerular or Bowman’s capsule, which surrounds the glomerulus, consists of a basement membrane, lined on its inner surface by a layer of flattened epithelial cells, which are reflected from the lining membrane on to the glomerulus, at the point of entrance or exit of the afferent and efferent vessels. The whole surface of the glomerulus is covered with a continuous layer of the same cells, on a delicate supporting membrane (Fig. 1130). Thus between the glomerulus and the capsule a space is left, forming a cavity lined by a continuous layer of squamous cells; this cavity varies in size according to the state of secretion and the amount of fluid present in it. In the fetus and young subject the lining epithelial cells are polyhedral or even columnar. | 20 |
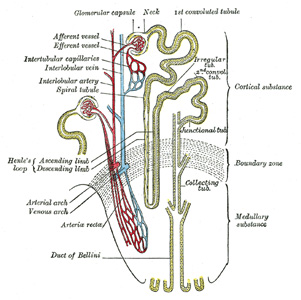 |
FIG. 1128– Scheme of renal tubule and its vascular supply. (See enlarged image) |
| |
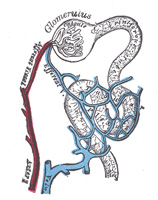 |
FIG. 1129– Distribution of bloodvessels in cortex of kidney. (See enlarged image) |
| |
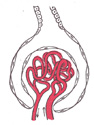 |
FIG. 1130– Glomerulus. (See enlarged image) |
| |
| The renal tubules, commencing in the renal corpuscles, present, during their course, many changes in shape and direction, and are contained partly in the medullary and partly in the cortical substance. At their junction with the glomerular capsule they exhibit a somewhat constricted portion, which is termed the neck. Beyond this the tubule becomes convoluted, and pursues a considerable course in the cortical substance constituting the proximal convoluted tube. After a time the convolutions disappear, and the tube approaches the medullary substance in a more or less spiral manner; this section of the tubule has been called the spiral tube. Throughout this portion of their course the renal tubules are contained entirely in the cortical substance, and present a fairly uniform caliber. They now enter the medullary substance, suddenly become much smaller, quite straight in direction, and dip down for a variable depth into the pyramids, constituting the descending limb of Henle’s loop. Bending on themselves, they form what is termed the loop of Henle, and reascending, they become suddenly enlarged, forming the ascending limb of Henle’s loop, and reënter the cortical substance. This portion of the tubule ascends for a short distance, when it again becomes dilated, irregular, and angular. This section is termed the zigzag tubule; it ends in a convoluted tube, which resembles the proximal convoluted tubule, and is called the distal convoluted tubule. This again terminates in a narrow junctional tube, which enters the straight or collecting tube. | 21 |
| The straight or collecting tubes commence in the radiate part of the cortex, where they receive the curved ends of the distal convoluted tubules. They unite at short intervals with one another, the resulting tubes presenting a considerable increase in caliber, so that a series of comparatively large tubes passes from the bases of the rays into the renal pyramids. In the medulla the tubes of each pyramid converge to join a central tube (duct of Bellini) which finally opens on the summit of one of the papillæ; the contents of the tube are therefore discharged into one of the calyces. | 22 |
| Structure of the Renal Tubules.—The renal tubules consist of a basement membrane lined with epithelium. The epithelium varies considerably in different sections of the tubule. In the neck the epithelium is continuous with that lining the glomerular capsule, and like it consists of flattened cells each containing an oval nucleus (Fig. 1132). The two convoluted tubules, the spiral and zigzag tubules and the ascending limb of Henle’s loop, are lined by a type of epithelium which is histologically the same in all. The cells are somewhat columnar in shape and dovetail into one another of their lateral aspect. Each has a striated border next the lumen of the tube, its inner part is granular and its outer portion vertically striated. The nucleus is spherical and situated about the center of the cell. In the descending limb of Henle’s loop the epithelium resembles that found in the glomerular capsule and the commencement of the tube, consisting of flat, clear epithelial plates, each with an oval nucleus (Fig. 1131). The nuclei alternate on opposite surfaces of the tubule so that the lumen remains fairly constant. | 23 |
| In the straight tube the epithelium is clear and cubical: in its papillary portion the cells are distinctly columnar and transparent (Fig. 1132). | 24 |
| |
| The Renal Bloodvessels.—The kidney is plentifully supplied with blood (Fig. 1133) by the renal artery, a large branch of the abdominal aorta. Before it enters the kidney, each artery divides into four or five branches which at the hilum lie mainly between the renal vein and ureter, the vein being in front, the ureter behind; one branch usually lies behind the ureter. Each vessel gives off some small branches to the suprarenal glands, to the ureter, land to the surrounding cellular tissue and muscles. Frequently a second renal artery, termed the inferior renal, is given off from the abdominal aorta at a lower level, and supplies the lower portion of the kidney, while occasionally an additional artery enters the upper part of the kidney. The branches of the renal artery, while in the sinus, give off a few twigs for the nutrition of the surrounding tissues, and end in the arteriæ propriæ renales, which enter the kidney proper in the renal columns. Two of these pass to each renal pyramid, and run along its sides for its entire length, giving off in their course the afferent vessels of the renal corpuscles in the renal columns. Having arrived at the bases of the pyramids, they form arterial arches or arcades which lie in the boundary zone between the bases of the pyramids and the cortical arches, and break up into two distinct sets of branches devoted to the supply of the remaining portions of the kidney. | 25 |
 |
FIG. 1131– Longitudinal section of descending limb of Henle’s loop. a. Membrana propria. b. Epithelium. (See enlarged image) |
| |
| The first set, the interlobular arteries (Fig. 1128), are given off at right angles from the side of the arterial arcade looking toward the cortical substance, and pass directly outward between the medullary rays to reach the fibrous tunic, where they end in the capillary net-work of this part. These vessels do not anastomose with each other, but form what are called end-arteries. In their outward course they give off lateral branches; these are the afferent vessels for the renal corpuscles (see page 1221); they enter the capsule, and end in the glomerulus. From each tuft the corresponding efferent vessel arises, and, having made its egress from the capsule near to the point where the afferent vessel enters, breaks up into a number of branches, which form a dense plexus around the adjacent urinary tubes. | 26 |
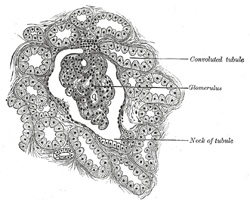 |
FIG. 1132– Section of cortex of human kidney. (See enlarged image) |
| |
| The second set of branches from the arterial arcades supply the renal pyramids, which they enter at their bases; and, passing straight through their substance to their apices, terminate in the venous plexuses found in that situation. They are called the arteriæ rectæ. The efferent vessels from the glomeruli nearest the medulla break up into leashes of straight vessels (false arteriæ rectæ) which pass down into the medulla and join the plexus of vessels there (Fig. 1128). | 27 |
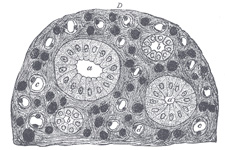 |
FIG. 1133– Transverse section of pyramidal substance of kidney of pig, the bloodvessels of which are injected. a. Large collecting tube, cut across, lined with cylindrical epithelium. b. Branch of collecting tube, cut across, lined with cubical epithelium. c, d. Henle’s loops cut across. e. Bloodvessels cut across. D. Connective tissue ground substance. (See enlarged image) |
| |
| The renal veins arise from three sources, viz., the veins beneath the fibrous tunic, the plexuses around the convoluted tubules in the cortex, and the plexuses situated at the apices of the renal pyramids. The veins beneath the fibrous tunic (venæ stellatæ) are stellate in arrangement, and are derived from the capillary net-work, into which the terminal branches of the interlobular arteries break up. These join to form the interlobular veins, which pass inward between the rays, receive branches from the plexuses around the convoluted tubules, and, having arrived at the bases of the renal pyramids, join with the venæ rectæ, next to be described. | 28 |
| The venæ rectæ are branches from the plexuses at the apices of the medullary pyramids, formed by the terminations of the arteriæ rectæ. They run outward in a straight course between the tubes of the medullary substance, and joining, as above stated, the interlobular veins, form venous arcades; these in turn unite and form veins which pass along the sides of the pyramids (Fig. 1128). | 29 |
| These vessels, venæ propriæ renales, accompany the arteries of the same name, running along the entire length of the sides of the pyramids, and quit the kidney substance to enter the sinus. In this cavity they join the corresponding veins from the other pyramids to form the renal vein, which emerges from the kidney at the hilum and opens into the inferior vena cava; the left vein is longer than the right, and crosses in front of the abdominal aorta. | 30 |
| The lymphatics of the kidney are described on page 712. | 31 |
| |
| Nerves of the Kidney.—The nerves of the kidney, although small, are about fifteen in number. They have small ganglia developed upon them, and are derived from the renal plexus, which is formed by branches from the celiac plexus, the lower and outer part of the celiac ganglion and aortic plexus, and from the lesser and lowest splanchnic nerves. They communicate with the spermatic plexus, a circumstance which may explain the occurrence of pain in the testis in affections of the kidney. They accompany the renal artery and its branches, and are distributed to the bloodvessels and to the cells of the urinary tubules. | 32 |
| |
| Connective Tissue (intertubular stroma).—Although the tubules and vessels are closely packed, a small amount of connective tissue, continuous with the fibrous tunic, binds them firmly together and supports the bloodvessels, lymphatics, and nerves. | 33 |
| |
| Variations.—Malformations of the kidney are not uncommon. There may be an entire absence of one kidney, but, according to Morris, the number of these cases is “excessively small”: or there may be congenital atrophy of one kidney, when the kidney is very small, but usually healthy in structure. These cases are of great importance, and must be duly taken into account when nephrectomy is contemplated. A more common malformation is where the two kidneys are fused together. They may be joined together only at their lower ends by means of a thick mass of renal tissue, so as to form a horseshoe-shaped body, or they may be completely united, forming a disk-like kidney, from which two ureters descend into the bladder. These fused kidneys are generally situated in the middle line of the abdomen, but may be misplaced as well. In some mammals, e. g., ox and bear, the kidney consists of a number of distinct lobules; this lobulated condition is characteristic of the kidney of the human fetus, and traces of it may persist in the adult. Sometimes the pelvis is duplicated, while a double ureter is not very uncommon. In some rare instances a third kidney may be present. | 34 |
| One or both kidneys may be misplaced as a congenital condition, and remain fixed in this abnormal position. They are then very often misshapen. They may be situated higher, though this is very uncommon, or lower than normal or removed farther from the vertebral column than usual; or they may be displaced into the iliac fossa, over the sacroiliac joint, on to the promontory of the sacrum, or into the pelvis between the rectum and bladder or by the side of the uterus. In these latter cases they may give rise to very serious trouble. The kidney may also be misplaced as a congenital condition, but may not be fixed; it is then known as a floating kidney. It is believed to be due to the fact that the kidney is completely enveloped by peritoneum which then passes backward to the vertebral column as a double layer, forming a mesonephron which permits movement. The kidney may also be misplaced as an acquired condition; in these cases the kidney is mobile in the tissues by which it is surrounded, moving with the capsule in the perinephric tissues. This condition is known as movable kidney, and is more common in the female than in the male. It occurs in badly nourished people, or in those who have become emaciated from any cause. It must not be confounded with the floating kidney, which is a congenital condition due to the development of a mesonephron. The two conditions cannot, however, be distinguished until the abdomen is opened or the kidney explored from the loin. | 35 |