| The jugular notch is in the same horizontal plane as the lower border of the body of the second thoracic vertebra; the sternal angle is at the level of the fifth thoracic vertebra, while the junction between the body and xiphoid process of the sternum corresponds to the fibrocartilage between the ninth and tenth thoracic vertebræ. | 2 |
| The influence of the obliquity of the ribs on horizontal levels in the thorax is well shown by the following line. “If a horizontal line be drawn around the body at the level of the inferior angle of the scapula, while the arms are at the sides, the line would cut the sternum in front between the fourth and fifth ribs, the fifth rib in the nipple line, and the ninth rib at the vertebral column.” (Treves). | 3 |
| |
| Diaphragm.—The shape and variations of the diaphragm as seen by skiagraphy have already been described (page 407). | 4 |
| |
| Surface Lines.—For clinical purposes, and for convenience of description, the surface of the thorax has been mapped out by arbitrary lines (Fig. 1220). On the front of the thorax the most important vertical lines are the midsternal, the middle line of the sternum; and the mammary, or, better midclavicular, which runs vertically downward from a point midway between the center of the jugular notch and the tip of the acromion. This latter line, if prolonged, is practically continuous with the lateral line on the front of the abdomen. Other vertical lines on the front of the thorax are the lateral sternal along the sternal margin, and the parasternal midway between the lateral sternal and the mammary. | 5 |
| On either side of the thorax the anterior and posterior axillary lines are drawn vertically from the corresponding axillary folds; the midaxillary line runs downward from the apex of the axilla. | 6 |
| On the posterior surface of the thorax the scapular line is drawn vertically through the inferior angle of the scapula. | 7 |
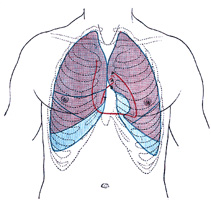 |
FIG. 1216– Front of thorax, showing surface relations of bones, lungs (purple), pleura (blue), and heart (red outline). P. Pulmonary valve. A. Aortic valve. B. Bicuspid valve. T. Tricuspid valve. (See enlarged image) |
| |
| |
| Pleuræ (Figs. 1216, 1217).—The lines of reflection of the pleuræ can be indicated on the surface. On the right side the line begins at the sternoclavicular articulation and runs downward and medialward to the midpoint of the junction between the manubrium and body of the sternum. It then follows the midsternal line to the lower end of the body of the sternum or on to the xiphoid process, where it turns lateralward and downward across the seventh sternocostal articulation. It crosses the eighth costochondral junction in the mammary line, the tenth rib in the midaxillary line, and is prolonged thence to the spinous process of the twelfth thoracic vertebra. | 8 |
| On the left side, beginning at the sternoclavicular articulation, it reaches the midpoint of the junction between the manubrium and body of the sternum and extends down the midsternal line in contact with that of the opposite side to the level of the fourth costal cartilage. It then diverges lateralward and is continued downward slightly lateral to the sternal border, as far as the sixth costal cartilage. Running downward and lateralward from this point it crosses the seventh costal cartilage, and from this onward it is similar to the line on the right side, but at a slightly lower level. | 9 |
| |
| Lungs (Figs. 1216, 1217).—The apex of the lung is situated in the neck above the medial third of the clavicle. The height to which it rises above the clavicle varies very considerably, but is generally about 2.5 cm. It may, however, extend as high as 4 or 5 cm., or, on the other hand, may scarcely project above the level of this bone. | 10 |
 |
FIG. 1217– Side of thorax, showing surface markings for bones, lungs (purple), pleura (blue), and spleen (green). (See enlarged image) |
| |
| In order to mark out the anterior borders of the lungs a line is drawn from each apex point—2.5 cm. above the clavicle and rather nearer the anterior than the posterior border of Sternocleidomastoideus—downward and medialward across the sternoclavicular articulation and manubrium sterni until it meets, or almost meets, its fellow of the other side at the midpoint of the junction between the manubrium and body of the sternum. From this point the two lines run downward, practically along the midsternal line, as far as the level of the fourth costal cartilages. The continuation of the anterior border of the right lung is marked by a prolongation of its line vertically downward to the level of the sixth costal cartilage, and then it turns lateralward and downward. The line on the left side curves lateralward and downward across the fourth sternocostal articulation to reach the parasternal line at the fifth costal cartilage, and then turns medialward and downward to the sixth sternocostal articulation. | 11 |
| In the position of expiration the lower border of the lung may be marked by a slightly curved line with its convexity downward, from the sixth sternocostal junction to the tenth thoracic spinous process. This line crosses the mid-clavicular line at the sixth, and the midaxillary line at the eighth rib. | 12 |
| The posterior borders of the lungs are indicated by lines drawn from the level of the spinous process of the seventh cervical vertebra, down either side of the vertebral column, across the costovertebral joints, as low as the spinous process of the tenth thoracic vertebra. | 13 |
| The position of the oblique fissure in either lung can be shown by a line drawn from the spinous process of the second thoracic vertebra around the side of the thorax to the sixth rib in the mid-clavicular line; this line corresponds roughly to the line of the vertebral border of the scapula when the hand is placed on the top of the head. The horizontal fissure in the right lung is indicated by a line drawn from the midpoint of the preceding, or from the point where it cuts the midaxillary line, to the midsternal line at the level of the fourth costal cartilage. | 14 |
| |
| Trachea.—This may be marked out on the back by a line from the spinous process of the sixth cervical to that of the fourth thoracic vertebra where it bifurcates; from its bifurcation the two bronchi are directed downward and lateralward. In front, the point of bifurcation corresponds to the sternal angle. | 15 |
| |
| Esophagus.—The extent of the esophagus may be indicated on the back by a line from the sixth cervical to the level of the ninth thoracic spinous process, 2.5 cm. to the left of the middle line. | 16 |
| |
| Heart.—The outline of the heart in relation to the front of the thorax (Figs 1216, 1218) can be represented by a quadrangular figure. The apex of the heart is first determined, either by its pulsation or as a point in the fifth interspace, 9 cm. to the left of the midsternal line. The other three points are: (a) the seventh right sternocostal articulation; (b) a point on the upper border of the third right costal cartilage 1 cm. from the right lateral sternal line; (c) a point on the lower border of the second left costal cartilage 2.5 cm. from the left lateral sternal line. A line joining the apex to point (a) and traversing the junction of the body of the sternum with the xiphoid process represents the lowest limit of the heart—its acute margin. The right and left borders are represented respectively by lines joining (a) to (b) and the apex to (c); both lines are convex lateralward, but the convexity is more marked on the right where its summit is 4 cm. distant from the midsternal line opposite the fourth costal cartilage. | 17 |
| A portion of the area of the heart thus mapped out is uncovered by lung, and therefore gives a dull note on percussion; the remainder being overlapped by lung gives a more or less resonant note. The former is known as the area of superficial cardiac dulness, the latter as the area of deep cardiac dulness. The area of superficial cardiac dulness is somewhat triangular; from the apex of the heart two lines are drawn to the midsternal line, one to the level of the fourth costal cartilage, the other to the junction between the body and xiphoid process; the portion of the midsternal line between these points is the base of the triangle. Latham lays down the following rule as a sufficient practical guide for the definition of the area of superficial dulness. “Make a circle of two inches in diameter around a point midway between the nipple and the end of the sternum.” | 18 |
| The coronary sulcus can be indicated by a line from the third left, to the sixth right, sternocostal joint. The anterior longitudinal sulcus is a finger’s breadth to the right of the left margin of the heart. | 19 |
| The position of the various orifices is as follows: The pulmonary orifice is situated in the upper angle of the third left sternocostal articulation; the aortic orifice is a little below and medial to this, close to the articulation. The left atrioventricular opening is opposite the fourth costal cartilage, and rather to the left of the midsternal line; the right atrioventricular opening is a little lower, opposite the fourth interspace of the right side. The lines indicating the atrioventricular openings are slightly below and parallel to the line of the coronary sulcus. | 20 |
| |
| Arteries.—The line of the ascending aorta begins slightly to the left of the midsternal line opposite the third costal cartilage and extends upward and to the right to the upper border of the second right costal cartilage. The beginning of the aortic arch is indicated by a line from this latter point to the midsternal line about 2.5 cm. below the jugular notch. The point on the midsternal line is opposite the summit of the arch, and a line from it to the right sternoclavicular articulation represents the site of the innominate artery, while another line from a point slightly to the left of it and passing through the left sternoclavicular articulation indicates the position of the left common carotid artery in the thorax. | 21 |
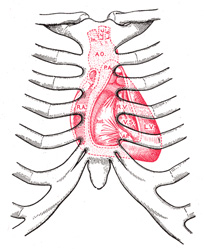 |
FIG. 1218– Diagram showing relations of opened heart to front of thoracic wall. Ant. Anterior segment of tricuspid valve. A O. Aorta. A.P. Anterior papillary muscle. In. Innominate artery. L.C.C. Left common carotid artery. L.S. Left subclavian artery. L.V. Left ventricle. P.A. Pulmonary artery. R.A. Right atrium. R.V. Right ventricle. V.S. Ventricular septum. (See enlarged image) |
| |
| The internal mammary artery descends behind the first six costal cartilages about 1 cm. from the lateral sternal line. | 22 |
| |
| Veins.—The line of the right innominate vein crosses the right sternoclavicular joint and the upper border of the first right costal cartilage about 1 cm. from the lateral sternal line; that of the left innominate vein extends from the left sternoclavicular articulation to meet the right at the upper border of the first right costal cartilage. The junction of the two lines indicates the origin of the superior vena cava, the line of which is continued vertically down to the level of the third right costal cartilage. The end of the inferior vena cava is situated opposite the upper margin of the sixth right costal cartilage about 2 cm. from the midsternal line. | 23 |