| The muscles belonging to this group are the | 1 |
| Intercostales externi. |
|
Levatores costarum. |
| Intercostales interni. |
|
Serratus posterior superior. |
| Subcostales. |
|
Serratus posterior inferior. |
| Transversus thoracis. |
|
Diaphragm. |
|
| |
| Intercostal Fasciæ.—In each intercostal space thin but firm layers of fascia cover the outer surface of the Intercostalis externus and the inner surface of the Intercostalis internus; and a third, more delicate layer, is interposed between the two planes of muscular fibers. They are best marked in those situations where the muscular fibers are deficient, as between the Intercostales externi and sternum in front, and between the Intercostales interni and vertebral column behind. | 2 |
| The Intercostales (Intercostal muscles) (Fig. 411) are two thin planes of muscular and tendinous fibers occupying each of the intercostal spaces. They are named external and internal from their surface relations—the external being superficial to the internal. | 3 |
| The Intercostales externi (External intercostals) are eleven in number on either side. They extend from the tubercles of the ribs behind, to the cartilages of the ribs in front, where they end in thin membranes, the anterior intercostal membranes, which are continued forward to the sternum. Each arises from the lower border of a rib, and is inserted into the upper border of the rib below. In the two lower spaces they extend to the ends of the cartilages, and in the upper two or three spaces they do not quite reach the ends of the ribs. They are thicker than the Intercostales interni, and their fibers are directed obliquely downward and lateralward on the back of the thorax, and downward, forward, and medialward on the front. | 4 |
| |
| Variations.—Continuation with the Obliquus externus or Serratus anterior: A Supracostalis muscle, from the anterior end of the first rib down to the second, third or fourth ribs occasionally occurs. | 5 |
| The Intercostales interni (Internal intercostals) are also eleven in number on either side. They commence anteriorly at the sternum, in the interspaces between the cartilages of the true ribs, and at the anterior extremities of the cartilages of the false ribs, and extend backward as far as the angles of the ribs, whence they are continued to the vertebral column by thin aponeuroses, the posterior intercostal membranes. Each arises from the ridge on the inner surface of a rib, as well as from the corresponding costal cartilage, and is inserted into the upper border of the rib below. Their fibers are also directed obliquely, but pass in a direction opposite to those of the Intercostales externi. | 6 |
| The Subcostales (Infracostales) consist of muscular and aponeurotic fasciculi, which are usually well-developed only in the lower part of the thorax; each arises from the inner surface of one rib near its angle, and is inserted into the inner surface of the second or third rib below. Their fibers run in the same direction as those of the Intercostales interni. | 7 |
| The Transversus thoracis (Triangularis sterni) is a thin plane of muscular and tendinous fibers, situated upon the inner surface of the front wall of the chest (Fig. 390). It arises on either side from the lower third of the posterior surface of the body of the sternum, from the posterior surface of the xiphoid process, and from the sternal ends of the costal cartilages of the lower three or four true ribs. Its fibers diverge upward and lateralward, to be inserted by slips into the lower borders and inner surfaces of the costal cartilages of the second, third, fourth, fifth, and sixth ribs. The lowest fibers of this muscle are horizontal in their direction, and are continuous with those of the Transversus abdominis; the intermediate fibers are oblique, while the highest are almost vertical. This muscle varies in its attachments, not only in different subjects, but on opposite sides of the same subject. | 8 |
| The Levatores costarum (Fig. 389), twelve in number on either side, are small tendinous and fleshy bundles, which arise from the ends of the transverse processes of the seventh cervical and upper eleven thoracic vertebræ; they pass obliquely downward and lateralward, like the fibers of the Intercostales externi, and each is inserted into the outer surface of the rib immediately below the vertebra from which it takes origin, between the tubercle and the angle (Levatores costarum breves). Each of the four lower muscles divides into two fasciculi, one of which is inserted as above described; the other passes down to the second rib below its origin (Levatores costarum longi). | 9 |
| The Serratus posterior superior (Serratus posticus superior) is a thin, quadrilateral muscle, situated at the upper and back part of the thorax. It arises by a thin and broad aponeurosis from the lower part of the ligamentum nuchae, from the spinous processes of the seventh cervical and upper two or three thoracic vertebræ and from the supraspinal ligament. Inclining downward and lateralward it becomes muscular, and is inserted, by four fleshy digitations, into the upper borders of the second, third, fourth, and fifth ribs, a little beyond their angles. | 10 |
| |
| Variations.—Increase or decrease in size and number of slips or entire absence. | 11 |
| The Serratus posterior inferior (Serratus posticus inferior) (Fig. 409) is situated at the junction of the thoracic and lumbar regions: it is of an irregularly quadrilateral form, broader than the preceding, and separated from it by a wide interval. It arises by a thin aponeurosis from the spinous processes of the lower two thoracic and upper two or three lumbar vertebræ, and from the supraspinal ligament. Passing obliquely upward and lateralward, it becomes fleshy, and divides into four flat digitations, which are inserted into the inferior borders of the lower four ribs, a little beyond their angles. The thin aponeurosis of origin is intimately blended with the lumbodorsal fascia, and aponeurosis of the Latissimus dorsi. | 12 |
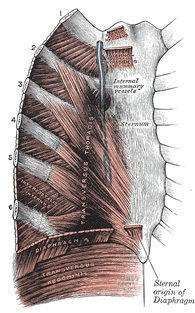 |
FIG. 390– Posterior surface of sternum and costal cartilages, showing Transversus thoracis. (See enlarged image) |
| |
| |
| Variations.—Increase or decrease in size and number of slips or entire absence. | 13 |
| |
| Nerves.—The muscles of this group are supplied by the intercostal nerves. | 14 |
| The Diaphragm (Fig. 391) is a dome-shaped musculofibrous septum which separates the thoracic from the abdominal cavity, its convex upper surface forming the floor of the former, and its concave under surface the roof of the latter. Its peripheral part consists of muscular fibers which take origin from the circumference of the thoracic outlet and converge to be inserted into a central tendon. | 15 |
| The muscular fibers may be grouped according to their origins into three parts—sternal, costal, and lumbar. The sternal part arises by two fleshy slips from the back of the xiphoid process; the costal part from the inner surfaces of the cartilages and adjacent portions of the lower six ribs on either side, interdigitating with the Transversus abdominis; and the lumbar part from aponeurotic arches, named the lumbocostal arches, and from the lumbar vertebræ by two pillars or crura. There are two lumbocostal arches, a medial and a lateral, on either side. | 16 |
| The Medial Lumbocostal Arch (arcus lumbocostalis medialis [Halleri]; internal arcuate ligament) is a tendinous arch in the fascia covering the upper part of the Psoas major; medially, it is continuous with the lateral tendinous margin of the corresponding crus, and is attached to the side of the body of the first or second lumbar vertebra; laterally, it is fixed to the front of the transverse process of the first and, sometimes also, to that of the second lumbar vertebra. | 17 |
| The Lateral Lumbocostal Arch (arcus lumbocostalis lateralis [Halleri]; external arcuate ligament) arches across the upper part of the Quadratus lumborum, and is attached, medially, to the front of the transverse process of the first lumbar vertebra, and, laterally, to the tip and lower margin of the twelfth rib. | 18 |
| |
| The Crura.—At their origins the crura are tendinous in structure, and blend with the anterior longitudinal ligament of the vertebral column. The right crus, larger and longer than the left, arises from the anterior surfaces of the bodies and intervertebral fibrocartilages of the upper three lumbar vertebræ, while the left crus arises from the corresponding parts of the upper two only. The medial tendinous margins of the crura pass forward and medialward, and meet in the middle line to form an arch across the front of the aorta; this arch is often poorly defined. | 19 |
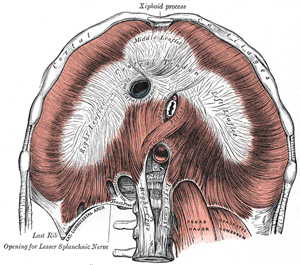 |
FIG. 391– The diaphragm. Under surface. (See enlarged image) |
| |
| From this series of origins the fibers of the diaphragm converge to be inserted into the central tendon. The fibers arising from the xiphoid process are very short, and occasionally aponeurotic; those from the medial and lateral lumbocostal arches, and more especially those from the ribs and their cartilages, are longer, and describe marked curves as they ascend and converge to their insertion. The fibers of the crura diverge as they ascend, the most lateral being directed upward and lateralward to the central tendon. The medial fibers of the right crus ascend on the left side of the esophageal hiatus, and occasionally a fasciculus of the left crus crosses the aorta and runs obliquely through the fibers of the right crus toward the vena caval foramen (Low 82). | 20 |
| |
| The Central Tendon.—The central tendon of the diaphragm is a thin but strong aponeurosis situated near the center of the vault formed by the muscle, but somewhat closer to the front than to the back of the thorax, so that the posterior muscular fibers are the longer. It is situated immediately below the pericardium, with which it is partially blended. It is shaped somewhat like a trefoil leaf, consisting of three divisions or leaflets separated from one another by slight indentations. The right leaflet is the largest, the middle, directed toward the xiphoid process, the next in size, and the left the smallest. In structure the tendon is composed of several planes of fibers, which intersect one another at various angles and unite into straight or curved bundles—an arrangement which gives it additional strength. | 21 |
| |
| Openings in the Diaphragm.—The diaphragm is pierced by a series of apertures to permit of the passage of structures between the thorax and abdomen. Three large openings—the aortic, the esophageal, and the vena caval—and a series of smaller ones are described. | 22 |
| The aortic hiatus is the lowest and most posterior of the large apertures; it lies at the level of the twelfth thoracic vertebra. Strictly speaking, it is not an aperture in the diaphragm but an osseoaponeurotic opening between it and the vertebral column, and therefore behind the diaphragm; occasionally some tendinous fibers prolonged across the bodies of the vertebræ from the medial parts of the lower ends of the crura pass behind the aorta, and thus convert the hiatus into a fibrous ring. The hiatus is situated slightly to the left of the middle line, and is bounded in front by the crura, and behind by the body of the first lumbar vertebra. Through it pass the aorta, the azygos vein, and the thoracic duct; occasionally the azygos vein is transmitted through the right crus. | 23 |
| The esophageal hiatus is situated in the muscular part of the diaphragm at the level of the tenth thoracic vertebra, and is elliptical in shape. It is placed above, in front, and a little to the left of the aortic hiatus, and transmits the esophagus, the vagus nerves, and some small esophageal arteries. | 24 |
| The vena caval foramen is the highest of the three, and is situated about the level of the fibrocartilage between the eighth and ninth thoracic vertebræ. It is quadrilateral in form, and is placed at the junction of the right and middle leaflets of the central tendon, so that its margins are tendinous. It transmits the inferior vena cava, the wall of which is adherent to the margins of the opening, and some branches of the right phrenic nerve. | 25 |
| Of the lesser apertures, two in the right crus transmit the greater and lesser right splanchnic nerves; three in the left crus give passage to the greater and lesser left splanchnic nerves and the hemiazygos vein. The gangliated trunks of the sympathetic usually enter the abdominal cavity behind the diaphragm, under the medial lumbocostal arches. | 26 |
| On either side two small intervals exist at which the muscular fibers of the diaphragm are deficient and are replaced by areolar tissue. One between the sternal and costal parts transmits the superior epigastric branch of the internal mammary artery and some lymphatics from the abdominal wall and convex surface of the liver. The other, between the fibers springing from the medial and lateral lumbocostal arches, is less constant; when this interval exists, the upper and back part of the kidney is separated from the pleura by areolar tissue only. | 27 |
| |
| Variations.—The sternal portion of the muscle is sometimes wanting and more rarely defects occur in the lateral part of the central tendon or adjoining muscle fibers. | 28 |
| |
| Nerves.—The diaphragm is supplied by the phrenic and lower intercostal nerves. | 29 |
| |
| Actions.—The diaphragm is the principal muscle of inspiration, and presents the form of a dome concave toward the abdomen. The central part of the dome is tendinous, and the pericardium is attached to its upper surface; the circumference is muscular. During inspiration the lowest ribs are fixed, and from these and the crura the muscular fibers contract and draw downward and forward the central tendon with the attached pericardium. In this movement the curvature of the diaphragm is scarcely altered, the dome moving downward nearly parallel to its original position and pushing before it the abdominal viscera. The descent of the abdominal viscera is permitted by the elasticity of the abdominal wall, but the limit of this is soon reached. The central tendon applied to the abdominal viscera then becomes a fixed point for the action of the diaphragm, the effect of which is to elevate the lower ribs and through them to push forward the body of the sternum and the upper ribs. The right cupola of the diaphragm, lying on the liver, has a greater resistance to overcome than the left, which lies over the stomach, but to compensate for this the right crus and the fibers of the right side generally are stronger than those of the left. | 30 |
| In all expulsive acts the diaphragm is called into action to give additional power to each expulsive effort. Thus, before sneezing, coughing, laughing, crying, or vomiting, and previous to the expulsion of urine or feces, or of the fetus from the uterus, a deep inspiration takes place. The height of the diaphragm is constantly varying during respiration; it also varies with the degree of distension of the stomach and intestines and with the size of the liver. After a forced expiration the right cupola is on a level in front with the fourth costal cartilage, at the side with the fifth, sixth, and seventh ribs, and behind with the eighth rib; the left cupola is a little lower than the right. Halls Dally 83 states that the absolute range of movement between deep inspiration and deep expiration averages in the male and female 30 mm. on the right side and 28 mm. on the left; in quiet respiration the average movement is 12.5 mm. on the right side and 12 mm. on the left. | 31 |
| Skiagraphy shows that the height of the diaphragm in the thorax varies considerably with the position of the body. It stands highest when the body is horizontal and the patient on his back, and in this position it performs the largest respiratory excursions with normal breathing. When the body is erect the dome of the diaphragm falls, and its respiratory movements become smaller. The dome falls still lower when the sitting posture is assumed, and in this position its respiratory excursions are smallest. These facts may, perhaps, explain why it is that patients suffering from severe dyspnœa are most comfortable and least short of breath when they sit up. When the body is horizontal and the patient on his side, the two halves of the diaphragm do not behave alike. The uppermost half sinks to a level lower even than when the patient sits, and moves little with respiration; the lower half rises higher in the thorax than it does when the patient is supine, and its respiratory excursions are much increased. In unilateral disease of the pleura or lungs analogous interference with the position or movement of the diaphragm can generally be observed skiagraphically. | 32 |
| It appears that the position of the diaphragm in the thorax depends upon three main factors, viz.: (1) the elastic retraction of the lung tissue, tending to pull it upward; (2) the pressure exerted on its under surface by the viscera; this naturally tends to be a negative pressure, or downward suction, when the patient sits or stands, and positive, or an upward pressure, when he lies; (3) the intra-abdominal tension due to the abdominal muscles. These are in a state of contraction in the standing position and not in the sitting; hence the diaphragm, when the patient stands, is pushed up higher than when he sits. | 33 |
| The Intercostales interni and externi have probably no action in moving the ribs. They contract simultaneously and form strong elastic supports which prevent the intercostal spaces being pushed out or drawn in during respiration. The anterior portions of the Intercostales interni probably have an additional function in keeping the sternocostal and interchondral joint surfaces in apposition, the posterior parts of the Intercostales externi performing a similar function for the costovertebral articulations. The Levatores costarum being inserted near the fulcra of the ribs can have little action on the ribs; they act as rotators and lateral flexors of the vertebral column. The Transversus thoracis draws down the costal cartilages, and is therefore a muscle of expiration. | 34 |
| The Serrati are respiratory muscles. The Serratus posterior superior elevates the ribs and is therefore an inspiratory muscle. The Serratus posterior inferior draws the lower ribs downward and backward, and thus elongates the thorax; it also fixes the lower ribs, thus assisting the inspiratory action of the diaphragm and resisting the tendency it has to draw the lower ribs upward and forward. It must therefore be regarded as a muscle of inspiration. | 35 |
| |
| Mechanism of Respiration.—The respiratory movements must be examined during (a) quiet respiration, and (b) deep respiration. | 36 |
| Quiet Respiration.—The first and second pairs of ribs are fixed by the resistance of the cervical structures; the last pair, and through it the eleventh, by the Quadratus lumborum. The other ribs are elevated, so that the first two intercostal spaces are diminished while the others are increased in width. It has already been shown (p. 304) that elevation of the third, fourth, fifth, and sixth ribs leads to an increase in the antero-posterior and transverse diameters of the thorax; the vertical diameter is increased by the descent of the diaphragmatic dome so that the lungs are expanded in all directions except backward and upward. Elevation of the eighth, ninth, and tenth ribs is accompanied by a lateral and backward movement, leading to an increase in the transverse diameter of the upper part of the abdomen; the elasticity of the anterior abdominal wall allows a slight increase in the antero-posterior diameter of this part, and in this way the decrease in the vertical diameter of the abdomen is compensated and space provided for its displaced viscera. Expiration is effected by the elastic recoil of its walls and by the action of the abdominal muscles, which push back the viscera displaced downward by the diaphragm. | 37 |
| Deep Respiration.—All the movements of quiet respiration are here carried out, but to a greater extent. In deep inspiration the shoulders and the vertebral borders of the scapulæ are fixed and the limb muscles, Trapezius, Serratus anterior, Pectorales, and Latissimus dorsi, are called into play. The Scaleni are in strong action, and the Sternocleidomastoidei also assist when the head is fixed by drawing up the sternum and by fixing the clavicles. The first rib is therefore no longer stationary, but, with the sternum, is raised; with it all the other ribs except the last are raised to a higher level. In conjunction with the increased descent of the diaphragm this provides for a considerable augmentation of all the thoracic diameters. The anterior abdominal muscles come into action so that the umbilicus is drawn upward and backward, but this allows the diaphragm to exert a more powerful influence on the lower ribs; the transverse diameter of the upper part of the abdomen is greatly increased and the subcostal angle opened out. The deeper muscles of the back, e.g., the Serrati posteriores superiores and the Sacrospinales and their continuations, are also brought into action; the thoracic curve of the vertebral column is partially straightened, and the whole column, above the lower lumbar vertebræ, drawn backward. This increases the antero-posterior diameters of the thorax and upper part of the abdomen and widens the intercostal spaces. Deep expiration is effected by the recoil of the walls and by the contraction of the antero-lateral muscles of the abdominal wall, and the Serrati posteriores inferiores and Transversus thoracis. | 38 |
| Halls Dally (op. cit.) gives the following figures as representing the average changes which occur during deepest possible respiration. The manubrium sterni moves 30 mm. in an upward and 14 mm. in a forward direction; the width of the subcostal angle, at a level of 30 mm. below the articulation between the body of the sternum and the xiphoid process, is increased by 26 mm.; the umbilicus is retracted and drawn upward for a distance of 13 mm. | 39 |