| The aorta is the main trunk of a series of vessels which convey the oxygenated blood to the tissues of the body for their nutrition. It commences at the upper part of the left ventricle, where it is about 3 cm. in diameter, and after ascending for a short distance, arches backward and to the left side, over the root of the left lung; it then descends within the thorax on the left side of the vertebral column, passes into the abdominal cavity through the aortic hiatus in the diaphragm, and ends, considerably diminished in size (about 1.75 cm. in diameter), opposite the lower border of the fourth lumbar vertebra, by dividing into the right and left common iliac arteries. Hence it is described in several portions, viz., the ascending aorta, the arch of the aorta, and the descending aorta, which last is again divided into the thoracic and abdominal aortæ. | 1 |
| |
| the Ascending Aorta (Aorta Ascendens) (Fig. 505).—The ascending aorta is about 5 cm. in length. It commences at the upper part of the base of the left ventricle, on a level with the lower border of the third costal cartilage behind the left half of the sternum; it passes obliquely upward, forward, and to the right, in the direction of the heart’s axis, as high as the upper border of the second right costal cartilage, describing a slight curve in its course, and being situated, about 6 cm. behind the posterior surface of the sternum. At its origin it presents, opposite the segments of the aortic valve, three small dilatations called the aortic sinuses. At the union of the ascending aorta with the aortic arch the caliber of the vessel is increased, owing to a bulging of its right wall. This dilatation is termed the bulb of the aorta, and on transverse section presents a somewhat oval figure. The ascending aorta is contained within the pericardium, and is enclosed in a tube of the serous pericardium, common to it and the pulmonary artery. | 2 |
| |
| Relations.—The ascending aorta is covered at its commencement by the trunk of the pulmonary artery and the right auricula, and, higher up, is separated from the sternum by the pericardium, the right pleura, the anterior margin of the right lung, some loose areolar tissue, and the remains of the thymus; posteriorly, it rests upon the left atrium and right pulmonary artery. On the right side, it is in relation with the superior vena cava and right atrium, the former lying partly behind it; on the left side, with the pulmonary artery. | 3 |
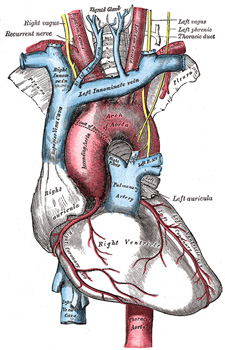 |
FIG. 505– The arch of the aorta, and its branches. (See enlarged image) |
| |
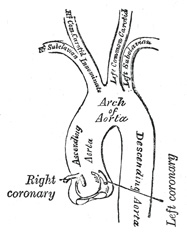 |
FIG. 506– Plan of the branches. (See enlarged image) |
| |
| |
| Branches.—The only branches of the ascending aorta are the two coronary arteries which supply the heart; they arise near the commencement of the aorta immediately above the attached margins of the semilunar valves. | 4 |
| |
| The Coronary Arteries.—The Right Coronary Artery (a. coronaria [cordis] dextra) arises from the right anterior aortic sinus. It passes at first between the conus arteriosus and the right auricula and then runs in the right portion of the coronary sulcus, coursing at first from the left to right and then on the diaphragmatic surface of the heart from right to left as far as the posterior longitudinal sulcus, down which it is continued to the apex of the heart as the posterior descending branch. It gives off a large marginal branch which follows the acute margin of the heart and supplies branches to both surfaces of the right ventricle. It also gives twigs to the right atrium and to the part of the left ventricle which adjoins the posterior longitudinal sulcus. | 5 |
| The Left Coronary Artery (a. coronaria [cordis] sinistra), larger than the right, arises from the left anterior aortic sinus and divides into an anterior descending and a circumflex branch. The anterior descending branch passes at first behind the pulmonary artery and then comes forward between that vessel and the left auricula to reach the anterior longitudinal sulcus, along which it descends to the incisura apicis cordis; it gives branches to both ventricles. The circumflex branch follows the left part of the coronary sulcus, running first to the left and then to the right, reaching nearly as far as the posterior longitudinal sulcus; it gives branches to the left atrium and ventricle. There is a free anastomosis between the minute branches of the two coronary arteries in the substance of the heart. | 6 |
| |
| Peculiarities.—These vessels occasionally arise by a common trunk, or their number may be increased to three, the additional branch being of small size. More rarely, there are two additional branches. | 7 |
| |
| The Arch of the Aorta (Arcus AortÆ; Transverse Aorta) (Fig. 505).—The arch of the aorta begins at the level of the upper border of the second sternocostal articulation of the right side, and runs at first upward, backward, and to the left in front of the trachea; it is then directed backward on the left side of the trachea and finally passes downward on the left side of the body of the fourth thoracic vertebra, at the lower border of which it becomes continuous with the descending aorta. It thus forms two curvatures: one with its convexity upward, the other with its convexity forward and to the left. Its upper border is usually about 2.5 cm. below the superior border to the manubrium sterni. | 8 |
| |
| Relations.—The arch of the aorta is covered anteriorly by the pleuræ and anterior margins of the lungs, and by the remains of the thymus. As the vessel runs backward its left side is in contact with the left lung and pleura. Passing downward on the left side of this part of the arch are four nerves; in order from before backward these are, the left phrenic, the lower of the superior cardiac branches of the left vagus, the superior cardiac branch of the left sympathetic, and the trunk of the left vagus. As the last nerve crosses the arch it gives off its recurrent branch, which hooks around below the vessel and then passes upward on its right side. The highest left intercostal vein runs obliquely upward and forward on the left side of the arch, between the phrenic and vagus nerves. On the right are the deep part of the cardiac plexus, the left recurrent nerve, the esophagus, and the thoracic duct; the trachea lies behind and to the right of the vessel. Above are the innominate, left common carotid, and left subclavian arteries, which arise from the convexity of the arch and are crossed close to their origins by the left innominate vein. Below are the bifurcation of the pulmonary artery, the left bronchus, the ligamentum arteriosum, the superficial part of the cardiac plexus, and the left recurrent nerve. As already stated, the ligamentum arteriosum connects the commencement of the left pulmonary artery to the aortic arch. | 9 |
| Between the origin of the left subclavian artery and the attachment of the ductus arteriosus the lumen of the fetal aorta is considerably narrowed, forming what is termed the aortic isthmus, while immediately beyond the ductus arteriosus the vessel presents a fusiform dilation which His has named the aortic spindle—the point of junction of the two parts being marked in the concavity of the arch by an indentation or angle. These conditions persist, to some extent, in the adult, where His found that the average diameter of the spindle exceeded that of the isthmus by 3 mm. | 10 |
| Distinct from this diffuse and moderate stenosis at the isthmus is the condition known as coarctation of the aorta, or marked stenosis often amounting to complete obliteration of its lumen, seen in adults and occuring at or near, oftenest a little below, the insertion of the ligamentum arteriosum into the aorta. According to Bonnet 96 this coarctation is never found in the fetus or at birth, and is due to an abnormal extension of the peculiar tissue of the ductus into the aortic wall, which gives rise to a simultaneous stenosis of both vessels as it contracts after birth—the ductus is usually obliterated in these cases. An extensive collateral circulation is set up, by the costocervicals, internal mammaries, and the descending branches of the transverse cervical above the stenosis, and below it by the first four aortic intercostals, the pericardiaco-phrenics, and the superior and inferior epigastrics. | 11 |
| |
| Peculiarities.—The height to which the aorta rises in the thorax is usually about 2.5 cm. below the upper border of the sternum; but it may ascend nearly to the top of the bone. Occasionally it is found 4 cm., more rarely from 5 to 8 cm. below this point. Sometimes the aorta arches over the root of the right lung (right aortic arch) instead of over that of the left, and passes down on the right side of the vertebral column, a condition which is found in birds. In such cases all the thoracic and abdominal viscera are transposed. Less frequently the aorta, after arching over the root of the right lung, is directed to its usual position on the left side of the vertebral column; this peculiarity is not accompanied by transposition of the viscera. The aorta occasionally divides, as in some quadrupeds, into an ascending and a descending trunk, the former of which is directed vertically upward, and subdivides into three branches, to supply the head and upper extremities. Sometimes the aorta subdivides near its origin into two branches, which soon reunite. In one of these cases the esophagus and trachea were found to pass through the interval between the two branches; this is the normal condition of the vessel in the reptilia. | 12 |
| |
| Branches (Figs. 505, 506).—The branches given off from the arch of the aorta are three in number: the innominate, the left common carotid, and the left subclavian. | 13 |
| |
| Peculiarities.—Position of the Branches.—The branches, instead of arising from the highest part of the arch, may spring from the commencement of the arch or upper part of the ascending aorta; or the distance between them at their origins may be increased or diminished, the most frequent change in this respect being the approximation of the left carotid toward the innominate artery. | 14 |
| The number of the primary branches may be reduced to one, or more commonly two; the left carotid arising from the innominate artery; or (more rarely) the carotid and subclavian arteries of the left side arising from a left innominate artery. But the number may be increased to four, from the right carotid and subclavian arteries arising directly from the aorta, the innominate being absent. In most of these latter cases the right subclavian has been found to arise from the left end of the arch; in other cases it is the second or third branch given off, instead of the first. Another common form in which there are four primary branches is that in which the left vertebral artery arises from the arch of the aorta between the left carotid and subclavian arteries. Lastly, the number of trunks from the arch may be increased to five or six; in these instances, the external and internal carotids arise separately from the arch, the common carotid being absent on one or both sides. In some few cases six branches have been found, and this condition is associated with the origin of both vertebral arteries from the arch. | 15 |
| |
| Number Usual, Arrangement Different.—When the aorta arches over to the right side, the three branches have an arrangement the reverse of what is usual; the innominate artery is a left, one, and the right carotid and subclavian arise separately. In other cases, where the aorta takes its usual course, the two carotids may be joined in a common trunk, and the subclavians arise separately from the arch, the right subclavian generally arising from the left end of the arch. | 16 |
| In some instances other arteries spring from the arch of the aorta. Of these the most common are the bronchial, one or both, and the thyreoidea ima; but the internal mammary and the inferior thyroid have been seen to arise from this vessel. | 17 |
| |
| The Innominate Artery (A. Anonyma; Brachiocephalic Artery) (Fig. 505).—The innominate artery is the largest branch of the arch of the aorta, and is from 4 to 5 cm. in length. It arises, on a level with the upper border of the second right costal cartilage, from the commencement of the arch of the aorta, on a plane anterior to the origin of the left carotid; it ascends obliquely upward, backward, and to the right to the level of the upper border of the right sternoclavicular articulation, where it divides into the right common carotid and right subclavian arteries. | 18 |
| |
| Relations.—Anteriorly, it is separated from the manubrium sterni by the Sternohyoideus and Sternothyreoideus, the remains of the thymus, the left innominate and right inferior thyroid veins which cross its root, and sometimes the superior cardiac branches of the right vagus. Posterior to it is the trachea, which it crosses obliquely. On the right side are the right innominate vein, the superior vena cava, the right phrenic nerve, and the pleura; and on the left side, the remains of the thymus, the origin of the left common carotid artery, the inferior thyroid veins, and the trachea. | 19 |
| |
| Branches.—The innominate artery usually gives off no branches; but occasionally a small branch, the thyreoidea ima, arises from it. Sometimes it gives off a thymic or bronchial branch. | 20 |
| The thyreoidea ima (a. thyreoidea ima) ascends in front of the trachea to the lower part of the thyroid gland, which it supplies. It varies greatly in size, and appears to compensate for deficiency or absence of one of the other thyroid vessels. It occasionally arises from the aorta, the right common carotid, the subclavian or the internal mammary. | 21 |
| |
| Point of Division.—The innominate artery sometimes divides above the level of the sternoclavicular joint, less frequently below it. | 22 |
| |
| Position.—When the aortic arch is on the right side, the innominate is directed to the left side of the neck. | 23 |
| |
| Collateral Circulation.—Allan Burns demonstrated, on the dead subject, the possibility of the establishment of the collateral circulation after ligature of the innominate artery, by tying and dividing that artery. He then found that “Even coarse injection, impelled into the aorta, passed freely by the anastomosing branches into the arteries of the right arm, filling them and all the vessels of the head completely.” 97 The branches by which this circulation would be carried on are very numerous; thus, all the communications across the middle line between the branches of the carotid arteries of opposite sides would be available for the supply of blood to the right side of the head and neck; while the anastomosis between the costocervical of the subclavian and the first aortic intercostal (see infra on the collateral circulation after obliteration of the thoracic aorta) would bring the blood, by a free and direct course, into the right subclavian. The numerous connections, also, between the intercostal arteries and the branches of the axillary and internal mammary arteries would, doubtless, assist in the supply of blood to the right arm, while the inferior epigastric from the external iliac would, by means of its anastomosis with the internal mammary, compensate for any deficiency in the vascularity of the wall of the chest. | 24 |