XII. Surface Anatomy and Surface Markings |
| |
| |
| 1. Surface Anatomy of the Head and Neck |
| |
| |
| Bones (Fig. 1193).—Various bony surfaces and prominences on the skull can be easily identified by palpation. The external occipital protuberance is situated behind, in the middle line, at the junction of the skin of the neck with that of the head. The superior nuchal line runs lateralward from it on either side, while extending downward from it is the median nuchal crest, situated deeply at the bottom of the nuchal furrow. Above the superior nuchal lines the vault of the cranium is thinly covered with soft structures, so that the form of this part of the head is almost that of the upper portion of the occipital, the parietal, and the frontal bones. The superior nuchal line can be followed lateralward to the mastoid portion of the temporal bone, from which the mastoid process projects downward and forward behind the ear. The anterior and posterior borders, the apex, and the external surface of this process are all available for superficial examination. The anterior border lies immediately behind the concha, and the apex is on a level with the lobule of the auricula. About 1 cm. below and in front of the apex of the mastoid process, the transverse process of the atlas can be distinguished. In front of the ear the zygomatic arch can be felt throughout its entire length; its posterior end is narrow and is situated a little above the level of the tragus; its anterior end is broad and is continued into the zygomatic bone. The lower border of the arch is more distinct than the upper, which is obscured by the attachment of the temporal fascia. In front, and behind, the upper border of the arch can be followed into the superior temporal line. In front, this line begins at the zygomatic process of the frontal bone as a curved ridge which runs at first forward and upward on the frontal bone, and then curving backward separates the forehead from the temporal fossa. It can then be traced across the parietal bone, where, though less marked, it can generally be recognized. Finally, it curves downward, and forward, and passing above the external acoustic meatus, ends in the posterior root of the zygomatic arch. Near the line of the greatest transverse diameter of the head are the parietal eminences, one on either side of the middle line; further forward, on the forehead, are the frontal eminences, which vary in prominence in different individuals and are frequently unsymmetrical. Below the frontal eminences the superciliary arches, which indicate the position of the frontal sinuses, can be recognized; as a rule they are small in the female and absent in children. In some cases the prominence of the superciliary arches is related to the size of the frontal sinuses, but frequently there is no such relationship. Situated between, and connecting the superciliary ridges, is a smooth, somewhat triangular area, the glabella, below which the nasion (frontonasal suture) can be felt as a slight depression at the root of the nose. | 1 |
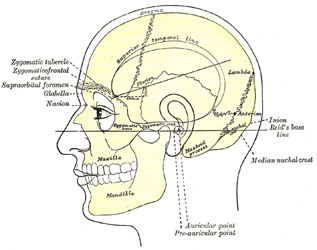 |
FIG. 1193– Side view of head, showing surface relations of bones. (See enlarged image) |
| |
| Below the nasion the nasal bones, scantily covered by soft tissues, can be traced to their junction with the nasal cartilages, and on either side of the nasal bone the complete outline of the orbital margin can be made out. At the junction of the medial and intermediate thirds of the supraorbital margin the supraorbital notch, when present, can be felt; close to the medial end of the infraorbital margin is a little tubercle which serves as a guide to the position of the lacrimal sac. Below and lateral to the orbit, on either side, is the zygomatic bone forming the prominence of the cheek; its posterior margin is easily palpable, and on it just above the level of the lateral palpebral commissure is the zygomatic tubercle. A slight depression, about 1 cm. above this tubercle, indicates the position of the zygomaticofrontal suture. Directly below the orbit a considerable part of the anterior surface of the maxilla and the whole of its alveolar process can be palpated. The outline of the mandible can be recognized throughout practically its entire extent; in front of the tragus and below the zygomatic arch is the condyle, and from this the posterior border of the ramus can be followed to the angle; from the angle to the symphysis the lower rounded border of the mandible can be easily traced; the lower part of the anterior border of the ramus and the alveolar process can be made out without difficulty. In the receding angle below the chin is the hyoid bone, and the finger can be carried along the bone to the tip of the greater cornu, which is on a level with the angle of the mandible: the greater cornu is most readily appreciated by making pressure on one side, when the cornu of the opposite side will be rendered prominent and can be felt distinctly beneath the skin. | 2 |
| |
| Joints and Muscles.—The temporomandibular articulation is quite superficial, and is situated below the posterior end of the zygomatic arch, in front of the external acoustic meatus. Its position can be ascertained by defining the condyle of the mandible; when the mouth opens, the condyle advances out of the mandibular fossa on to the articular tubercle, and a depression is felt in the situation of the joint. | 3 |
| The outlines of the muscles of the head and face cannot be traced on the surface except in the case of the Masseter and Temporalis. The muscles of the scalp are so thin that the outline of the bone is perceptible beneath them. Those of the face are small, covered by soft skin, and often by a considerable layer of fat, and their outlines are therefore concealed; they serve, however, to round off and smooth prominent borders, and to fill up what would otherwise be unsightly angular depressions. Thus the Orbicularis oculi rounds off the prominent margin of the orbit, and the Procerus fills in the sharp depression below the glabella. In like manner the labial muscles converging to the lips, and assisted by the superimposed fat, fill up the sunken hollow of the lower part of the face. When in action the facial muscles produce the various expressions, and in addition throw the skin into numerous folds and wrinkles. The Masseter imparts fulness to the hinder part of the cheek; if firmly contracted, as when the teeth are clenched, its quadrilateral outline is plainly visible; the anterior border forms a prominent vertical ridge, behind which is a considerable fulness especially marked at the lower part of the muscle. The Temporalis is fan-shaped and fills the temporal fossa, substituting for the concavity a somewhat convex swelling, the anterior part of which, on account of the absence of hair on the overlying skin, is more marked than the posterior, and stands out in strong relief when the muscle is in action. | 4 |
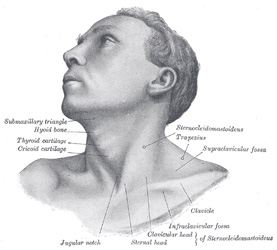 |
FIG. 1194– Anterolateral view of head and neck. (See enlarged image) |
| |
| In the neck, the Platysma when contracted throws the skin into oblique ridges parallel with the fasciculi of the muscle. The Sternocleidomastoideus has the most important influence on the surface form of the neck (Figs. 1194, 1195). When the muscle is at rest its anterior border forms an oblique rounded edge ending below in the sharp outline of the sternal head; the posterior border is only distinct for about 2 or 3 cm. above the middle of the clavicle. During contraction, the sternal head stands out as a sharply defined ridge, while the clavicular head is flatter and less prominent; between the two heads is a slight depression: the fleshy middle portion of the muscle appears as an oblique elevation with a thick, rounded, anterior border, best marked in its lower part. The sternal heads of the two muscles are separated by a V-shaped depression, in which are the Sternohyoideus and Sternothyreoideus. | 5 |
| Above the hyoid bone, near the middle line, the anterior belly of the Digastricus produces a slight convexity. | 6 |
| The anterior border of the Trapezius presents as a faint ridge running from the superior nuchal line, downward and forward to the junction of the intermediate and lateral thirds of the clavicle. Between the Sternocleidomastoideus and the Trapezius is the posterior triangle of the neck, the lower part of which appears as a shallow concavity—the supraclavicular fossa. In this fossa, the inferior belly of the Omohyoideus, when in action, presents as a rounded cord-like elevation a little above, and almost parallel to, the clavicle. | 7 |
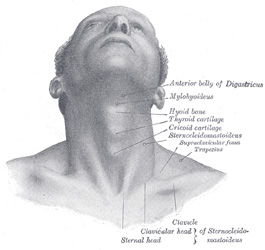 |
FIG. 1195– Front view of neck. (See enlarged image) |
| |
| |
| Arteries.—The positions of several of the larger arteries can be ascertained from their pulsations. | 8 |
| The subclavian artery can be felt by making pressure downward, backward, and medialward behind the clavicular head of the Sternocleidomastoideus; its transverse cervical branch may be detected parallel to, and about a finger’s breadth above, the clavicle. The common and external carotid arteries can be recognized immediately beneath the anterior edge of the Sternocleidomastoideus. The external maxillary artery can be traced over the border of the mandible just in front of the anterior border of the Masseter, then about 1 cm. lateral to the angle of the mouth, and finally as it runs up the side of the nose. The pulsation of the occipital artery can be distinguished about 3 or 4 cm. lateral to the external occipital protuberance; that of the posterior auricular in the groove between the mastoid process and the auricula. The course of the superficial temporal artery can be readily followed across the posterior end of the zygomatic arch to a point about 3 to 5 cm. above this, where it divides into its frontal and parietal branches; the pulsation of the frontal branch is frequently visible on the side of the forehead. The supraorbital artery can usually be detected immediately above the supraorbital notch or foramen. | 9 |