| Auricular Point.—The center of the orifice of the external acoustic meatus. | 3 |
| Preauricular Point.—A point on the posterior root of the zygomatic arch immediately in front of the external acoustic meatus. | 4 |
| Asterion.—The point of meeting of the lambdoidal, mastoöccipital, and mastoparietal sutures; it lies 4 cm. behind and 12 mm. above the level of the auricular point. | 5 |
| Pterion.—The point where the great wing of the sphenoid joins the sphenoidal angle of the parietal; it is situated 35 mm. behind, and 12 mm. above, the level of the frontozygomatic suture. | 6 |
| Inion.—The external occipital protuberance. | 7 |
| Lambda.—The point of meeting of the lambdoidal and sagittal sutures; it is in the middle line about 6.5 cm. above the inion. | 8 |
| Bregma.—The meeting-point of the coronal and sagittal sutures; it lies at the point of intersection of the middle line of the scalp with a line drawn vertically upward through the preauricular point. | 9 |
| A line passing through the inferior margin of the orbit and the auricular point is known as Reid’s base line. The lambdoidal suture can be indicated on either side by the upper two-thirds of a line from the lambda to the tip of the mastoid process. The sagittal suture is in the line joining the lambda to the bregma. The position of the coronal suture on either side is sufficiently represented by a line joining the bregma to the center of the zygomtic arch. | 10 |
| The floor of the middle fossa of the skull is at the level of the posterior three-fourths of the upper border of the zygomatic arch; the articular eminence of the temporal bone is opposite the foramen spinosum and the semilunar ganglion. | 11 |
 |
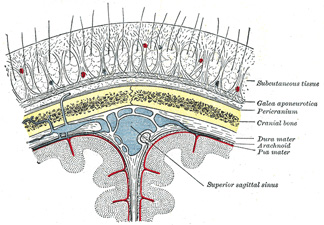
FIG. 1197– Drawing of a cast by Cunningham to illustrate the relations of the brain to the skull. (See enlarged image) |
| |
| |
| Brain (Figs. 1197, 1198).—The general outline of the cerebral hemisphere, on either side, may be mapped out on the surface in the following manner. Starting from the nasion, a line drawn along the middle of the scalp to the inion represents the superior border. The line of the lower margin behind is that of the transverse sinus (see page 1294), or more roughly a line convex upward from the inion to the posterior root of the zygomatic process of the temporal bone; thence along the posterior two-thirds of the upper border of the zygomatic arch where the line turns up to the pterion; the front part of the lower margin extends from the pterion to the glabella about 1 cm. above the supraorbital margin. The cerebellum is so deeply situated that there is no reliable surface marking for it; a point 4 cm. behind and 1.5 cm. below the level of the auricular point is situated directly over it. | 12 |
| The relations of the principal fissures and gyri of the cerebral hemispheres to the surface of the scalp are of considerable practical importance, and several methods of indicating them have been devised. Necessarily these methods can only be regarded as approximately correct, yet they are all sufficiently accurate for surgical purposes. The longitudinal fissure corresponds to the medial line of the scalp between the nasion and inion. In order to mark out the lateral cerebral (Sylvian) fissure a point, termed the Sylvian point, which practically corresponds to the pterion, is defined 35 mm. behind and 12 mm. above the level of the frontozygomatic suture; this point marks the spot where the lateral fissure divides. Another method of defining the Sylvian point is to divide the distance between the nasion and inion into four equal parts; from the junction of the third and fourth parts (reckoning from the front) draw a line to the frontozygomatic suture; from the junction of the first and second parts a line to the auricular point. These two lines intersect at the Sylvian point and the portion of the first line behind this point overlies the posterior ramus of the lateral cerebral fissure. The position of the posterior ramus can otherwise be obtained by joining the Sylvian point to a point 2 cm. below the summit of the parietal eminence. The anterior ascending ramus can be marked out by drawing a line upward at right angles to the line of the posterior ramus for 2 cm. and the anterior horizontal ramus by a line of the same length drawn horizontally forward—both from the Sylvian point. To define the central sulcus (fissure of Rolando) two points are taken; one is situated 1.25 cm. behind the center of the line joining the nasion and inion; the second is at the intersection of the line of the posterior ramus of the lateral cerebral fissure with a line through the preauricular point at right angles to Reid’s base line. The upper 9 cm. of the line joining these two points overlies the central sulcus and forms an angle, opening forward, of about 70° with the middle line of the scalp. An alternative method is to draw two perpendicular lines from Reid’s base line to the top of the head; one from the preauricular point and the other from the posterior border of the mastoid process at its root. A line from the upper end of the posterior line to the point where the anterior intersects the line of the posterior ramus of the lateral fissure indicates the position of the central sulcus. The precetral and postcentral sulci are practically parallel to the central sulcus; they are situated respectively about 15 mm. in front of, and behind, it. The superior frontal sulcus can be mapped out by a line drawn from the junction of the upper and middle thirds of the precentral sulcus, in a direction parallel with the longitudinal sulcus, to a point midway between the middle line of the forehead and the temporal line, 4 cm. above the supraorbital notch. The inferior frontal sulcus begins at the junction of the middle and lower thirds of the precentral sulcus, and follows the course of the superior temporal line. | 13 |
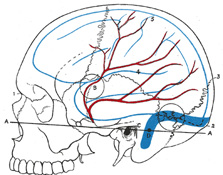 |
FIG. 1198– Relations of the brain and middle meningeal artery to the surface of the skull. 1. Nasion. 2. Inion. 3. Lambda. 4. Lateral cerebral fissure. 5. Central sulcus. AA. Reid’s base line. B. Point for trephining the anterior branch of the middle meningeal artery. C. Suprameatal triangle. D. Sigmoid bend of the transverse sinus. E. Point for trephining over the straight portion of the transverse sinus, exposing dura mater of both cerebrum and cerebellum. Outline of cerebral hemisphere indicated in blue; course of middle meningeal artery in red. (See enlarged image) |
| |
| The horizontal limb of the intraparietal sulcus begins from the junction of the lower with the middle third of the postcentral sulcus and curves backward parallel to the longitudinal fissure, midway between it and the parietal eminence; it then curves downward to end midway between the lambda and the parietal eminence. The external part of the parietoöccipital fissure runs lateralward at right angles to the longitudinal fissure for about 2.5 cm. from a point 5 mm. in front of the lambda. If the line of the posterior ramus of the lateral cerebral fissure be continued back to the longitudinal fissure, the last 2.5 cm. of it will indicate the position of the parietoöccipital fissure. | 14 |
| The lateral ventricle may be circumscribed by a quadrilateral figure. The upper limit is a horizontal line 5 cm. above the zygomatic arch; this defines the roof of the ventricle. The lower limit is a horizontal line 1 cm. above the zygomatic arch; it indicates the level of the end of the inferior horn. Two vertical lines, one through the junction of the anterior and middle thirds of the zygomatic arch, and the other 5 cm. behind the tip of the mastoid process, indicate the extent of the anterior horn in front and the posterior horn behind. | 15 |
| |
| Vessels.—The line of the anterior division of the middle meningeal artery is equidistant from the frontozygomatic suture and the zygomatic arch; it is obtained by joining up the following points: (1) 2.5 cm., (2) 4 cm., and (3) 5 cm. from these two landmarks. The posterior division can be reached 2.5 cm. above the auricular point. | 16 |
| The position of the transverse sinus is obtained by taking two lines: the first from the inion to a point 2.5 cm. behind the auricular point; the second from the anterior end of the first to the tip of the mastoid process. The second line corresponds roughly to the line of reflection of the skin of the auricula behind, and its upper two-thirds represents the sigmoid part of the sinus. The first part of the sinus has a slight upward convexity, and its highest point is about 4 cm. behind and 1 cm. above the level of the auricular point. The width of the sinus is about 1 cm. | 17 |
| |
| The Face.—Air Sinuses (Fig. 1199).—The frontal and maxillary sinuses vary so greatly in form and size that their surface markings must be regarded as only roughly approximate. To mark out the position of the frontal sinus three points are taken: (1) the nasion, (2) a point in the middle line 3 cm. above the nasion, (3) a point at the junction of the lateral and intermediate thirds of the supraorbital margin. By joining these a triangular field is described which overlies the greater part of the sinus. The outline of the maxillary sinus is irregularly quadrilateral and is obtained by joining up the following points: (1) the lacrimal tubercle, (2) a point on the zygomatic bone at the level of the inferior and lateral margins of the orbit, (3) and (4) points on the alveolar process above the last molar and the second premolar teeth respectively. | 18 |
| |
| External Maxillary Artery.—The course of this artery on the face may be indicated by a line starting from the lower border of the mandible at the anterior margin of the Masseter, and running at first forward and upward to a point 1 cm. lateral to the angle of the mouth, thence to the ala of the nose and upward to the medial commissure of the eye (Fig. 1200). | 19 |
| |
| Trigeminal Nerve.—Terminal branches of this nerve, viz., the supraorbital branch of the ophthalmic, the infraorbital of the maxillary, and the mental of the mandibular emerge from corresponding foramina on the face (Fig. 1200). The supraorbital foramen is situated at the junction of the medial and intermediate thirds of the supraorbital margin. A line drawn from this foramen to the lower border of the mandible, through the interval between the two lower premolar teeth, passes over the infraorbital and mental foramina; the former lies about 1 cm. below the margin of the orbit, while the latter varies in position according to the age of the individual; in the adult it is midway between the upper and lower borders of the mandible, in the child it is nearer the lower border, while in the edentulous jaw of old age it is close to the upper margin. | 20 |
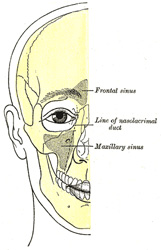 |
FIG. 1199– Outline of bones of face, showing position of air sinuses. (See enlarged image) |
| |
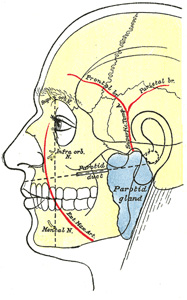 |
FIG. 1200– Outline of side of face, showing chief surface markings. (See enlarged image) |
| |
| The position of the sphenopalatine ganglion is indicated from the side by a point on the upper border of the zygomatic arch, 6 mm. from the margin of the zygomatic bone. | 21 |
| |
| Parotid Gland (Fig. 1200).—The upper border of the parotid gland corresponds to the posterior two-thirds of the lower border of the zygomatic arch; the posterior border to the front of the external acoustic meatus, the mastoid process, and the anterior border of Sternocleidomastoideus. The inferior border is indicated by a line from the tip of the mastoid process to the junction of the body and greater cornu of the hyoid bone. In front, the anterior border extends for a variable distance on the superficial surface of the Masseter. The surface marking for the parotid duct is a line drawn across the face about a finger’s breadth below the zygomatic arch, i. e., from the lower margin of the concha to midway between the red margin of the lip and the ala of the nose; the duct ends opposite the second upper molar tooth and measures about 5 cm. in length. | 22 |
| |
| The Nose.—The outlines of the nasal bones and the cartilages forming the external nose can be easily felt. The mobile portion of the nasal septum, formed by the medial crura of the greater alar cartilages and the skin, is easily distinguished between the nares. When the head is tilted back and a speculum introduced through the naris, the floor of the nasal cavity, the lower part of the nasal septum, and the anterior ends of the middle and inferior nasal conchæ can be examined. The opening of the nasolacrimal duct, which lies under cover of the front of the inferior nasal concha, is situated about 2.5 cm. behind the naris and 2 cm. above the level of the floor of the nasal cavity. | 23 |
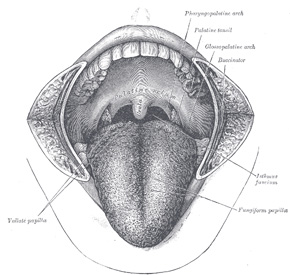 |
FIG. 1201– The mouth cavity. The cheeks have been slit transversely and the tongue pulled forward. (See enlarged image) |
| |
| |
| The Mouth.—The orifice of the mouth is bounded by the lips, which are covered externally by the whitish skin and internally by the red mucous membrane. The size of the orifice varies considerably in different individuals, but seems to bear a close relationship to the size and prominence of the teeth; its angles usually correspond to the lateral borders of the canine teeth. Running down the center of the outer surface of the upper lip is a shallow groove—the philtrum. If the lips be everted there can be seen, in the middle line of each, a small fold of mucous membrane—the frenulum—passing from the lip to the gum. By pulling the angle of the mouth outward the mucous membrane of the cheek can be inspected, and on this, opposite the second molar tooth of the maxilla, is the little papilla which marks the orifice of the parotid duct. | 24 |
| In the floor of the mouth is the tongue (Fig. 1201). Its upper surface is convex and is marked along the middle line by a shallow sulcus; the anterior two-thirds are rough and studded with papillæ; the posterior third is smooth and tuberculated. The division between the anterior two-thirds and the posterior third is marked by a V-shaped furrow, the sulcus terminalis, which is situated immediately behind the line of the vallate papillæ. | 25 |
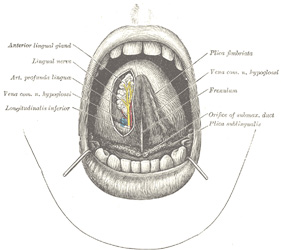 |
FIG. 1202– The mouth cavity. The apex of the tongue is turned upward, and on the right side a superficial dissection of its under surface has been made. (See enlarged image) |
| |
| On the under surface of the tongue (Fig. 1202) the mucous membrane is smooth and devoid of papillæ. In the middle line, the mucous membrane extends to the floor of the mouth as a distinct fold—the frenulum—the free edge of which runs forward to the symphysis menti. Sometimes the ranine vein can be seen immediately beneath the mucous membrane, a little lateral to the frenulum. Close to the attachment of the frenulum to the floor of the mouth, the slit-like orifice of the submaxillary duct is visible on either side. Running backward and lateralward from the orifice of the submaxillary duct is the plica sublingualis, produced by the projection of the sublingual gland which lies immediately beneath the mucous membrane. The plica serves also to indicate the line of the submaxillary duct and of the lingual nerve. At the back of the mouth is the isthmus faucium, bounded above by the palatine velum, from the free margin of which the uvula projects downward in the middle line. On either side of the isthmus are the two palatine arches, the anterior formed by the Glossopalatinus and the posterior by the Pharyngopalatinus. Between the two arches of either side is the palatine tonsil, above which is the small supratonsillar recess; the position of the tonsil corresponds to the angle of the mandible. When the mouth is opened widely, a tense band—the pterygomandibular raphé—can be seen and felt lateral to the glossopalatine arch. Its lower end is attached to the mandible behind the last molar tooth, and immediately below and in front of this the lingual nerve can be felt; the upper end of the ligament can be traced to the pterygoid hamulus. About 1 cm. in front of the hamulus and 1 cm. medial to the last molar tooth of the maxilla is the greater palatine foramen through which the descending palatine vessels and the anterior palatine nerve emerge. Behind the last molar tooth of the maxilla the coronoid process of the mandible is palpable. | 26 |
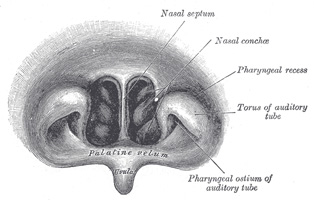 |
FIG. 1203– Front of nasal part of pharynx, as seen with the laryngoscope. (See enlarged image) |
| |
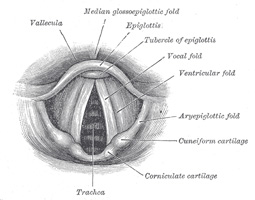 |
FIG. 1204– Laryngoscopic view of interior of larynx (See enlarged image) |
| |
| By tilting the head well back a portion of the posterior pharyngeal wall, corresponding to the site of the second and third cervical vertebræ, can be seen through the isthmus faucium. On introducing the finger the anterior surfaces of the upper cervical vertebræ can be felt through the thin muscular wall of the pharynx; if the finger be hooked round the palatine velum, the choanæ can be distinguished in front, and the pharyngeal ostium of the auditory tube on either side. The level of the choanæ is that of the atlas, while the palatine velum is opposite the body of the axis. | 27 |
| With the laryngoscope many other structures can be seen. In the nasal part of the pharynx (Fig. 1203), the choanæ, the nasal septum, the nasal conchæ, and the pharyngeal ostia of the auditory tubes can all be examined. Further down, the base of the tongue, the anterior surface of the epiglottis with the glossoepiglottic and pharyngoepiglottic folds bounding the valleculæ, and the piriform sinuses, are readily distinguished. Beyond these is the entrance to the larynx, bounded on either side by the aryepiglottic folds, in each of which are two rounded eminences corresponding to the corniculate and cuneiform cartilages. | 28 |
| Within the larynx (Fig. 1204) on either side are the ventricular and vocal folds (false and true vocal cords) with the ventricle between them. Still deeper are seen the cricoid cartilage and the anterior parts of some of the cartilaginous rings of the trachea, and sometimes, during deep inspiration, the bifurcation of the trachea. | 29 |
| |
| The Eye.—The palpebral fissure is elliptical in shape, and varies in form in different individuals and in different races of mankind; normally it is oblique, in a direction upward and lateralward, so that the lateral commissure is on a slightly higher level than the medial. When the eyes are directed forward as in ordinary vision the upper part of the cornea is covered by the upper eyelid and its lower margin corresponds to the level of the free margin of the lower eyelid, so that usually the lower three-fourths are exposed. | 30 |
| At the medial commissure (Fig. 1205) are the caruncula lacrimalis and the plica semilunaris. When the lids are everted, the tarsal glands appear as a series of nearly straight parallel rows of light yellow granules. On the margins of the lids about 5 mm. from the medial commissure are two small openings—the lacrimal puncta; in the natural condition they are in contact with the conjunctiva of the bulb of the eye, so that it is necessary to evert the eyelids to expose them. The position of the lacrimal sac is indicated by a little tubercle which can be plainly felt on the lower margin of the orbit; the sac lies immediately above and medial to the tubercle. If the eyelids be drawn lateralward so as to tighten the skin at the medial commissure a prominent core can be felt beneath the tightened skin; this is the medial palpebral ligament, which lies over the junction of the upper with the lower two-thirds of the sac, thus forming a useful guide to its situation. The direction of the nasolacrimal duct is indicated by a line from the lacrimal sac to the first molar tooth of the maxilla; the length of the duct is about 12 or 13 mm. | 31 |
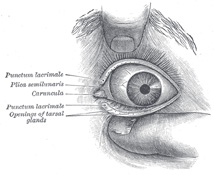 |
FIG. 1205– Front of left eye with eyelids separated to show medial canthus. (See enlarged image) |
| |
| On looking into the eye, the iris with its opening, the pupil, and the front of the lens can be examined, but for investigation of the retina an ophthalmoscope is necessary. With this the lens, the vessels of the retina, the optic disk, and the macula lutea can all be inspected (Fig. 1206). | 32 |
| On the lateral surface of the nasal part of the frontal bone the pulley of the Obliquus superior can be easily reached by pushing the finger backward along the roof of the orbit; the tendon of the muscle can be traced for a short distance backward and lateralward from the pulley. | 33 |
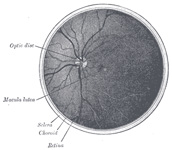 |
FIG. 1206– The interior of the posterior half of the left eyeball. (See enlarged image) |
| |
| |
| The Ear.—The various prominences and fossæ of the auricula (see page 1034) are visible (Fig. 1207). The opening of the external acoustic meatus is exposed by drawing the tragus forward; at the orifice are a few short crisp hairs which serve to prevent the entrance of dust or of small insects; beyond this the secretion of the ceruminous glands serves to catch any small particles which may find their way into the meatus. The interior of the meatus can be examined through a speculum. At the line of junction of its bony and cartilaginous portions an obtuse angle is formed which projects into the antero-inferior wall and produces a narrowing of the lumen in this situation. The cartilaginous part, however, is connected to the bony part by fibrous tissue which renders the outer part of the meatus very movable, and therefore by drawing the auricula upward, backward, and slightly outward, the canal is rendered almost straight. In children the meatus is very short, and this should be remembered in introducing the speculum. | 34 |
 |
FIG. 1207– The auricula or pinna. Lateral surface. (See enlarged image) |
| |
| Through the speculum the greater part of the tympanic membrane (Fig. 1208) is visible. It is a pearlygray membrane slightly glistening in the adult, placed obliquely so as to form with the floor of the meatus an angle of about 55°. At birth it is more horizontal and situated in almost the same plane as the base of the skull. The membrane is concave outward, and the point of deepest concavity—the umbo—is slightly below the center. Running upward and slightly forward from the umbo is a reddish-yellow streak produced by the manubrium of the malleus. This streak ends above just below the roof of the meatus at a small white rounded prominence which is caused by the lateral process of the malleus projecting against the membrane. The anterior and posterior malleolar folds extend from the prominence to the circumference of the membrane and enclose the pars flaccida. Behind the streak caused by the manubrium of the malleus a second streak, shorter and very faint, can be distinguished; this is the long crus of the incus. A narrow triangular patch extending downward and forward from the umbo reflects the light more brightly than any other part, and is usually described as the cone of light. | 35 |
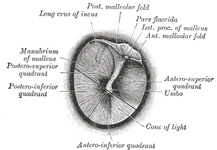 |
FIG. 1208– The right tympanic membrane as seen through a speculum. (See enlarged image) |
| |
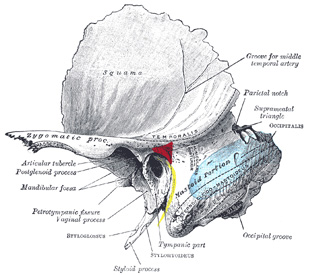 |
FIG. 1209– Left temporal bone showing surface markings for the tympanic antrum (red), transverse sinus (blue), and facial nerve (yellow). (See enlarged image) |
| |
| |
| Tympanic Antrum.—The site of the tympanic antrum is indicated by the suprameatal triangle (Fig. 1209). This triangle is bounded above by the posterior root of the zygomatic arch; behind by a vertical line from the posterior border of the external acoustic meatus; in front and below by the upper margin of the meatus. | 36 |
| |
| The Neck (Fig. 1210).—Larynx and Trachea.—In the receding angle below the chin, the hyoid bone (page 1288), situated opposite the fourth cervical vertebra, can easily be made out. A finger’s breadth below it is the laryngeal prominence of the thyroid cartilage; the space intervening between the hyoid bone and the thyroid cartilage is occupied by the hyothyroid membrane. The outlines of the thyroid cartilage are readily palpated; below its lower border is a depression corresponding to the middle cricothyroid ligament. The level of the vocal folds corresponds to the middle of the anterior margin of the thyroid cartilage. The anterior part of the cricoid cartilage forms an important landmark on the front of the neck; it lies opposite the sixth cervical vertebra, and indicates the junctions of pharynx with esophagus, and larynx with trachea. Below the cricoid cartilage the trachea can be felt, though it is only in thin subjects that the separate rings can be distinguished; as a rule there are seven or eight rings above the jugular notch of the sternum, and of these the second, third, and fourth are covered by the isthmus of the thyroid gland. | 37 |
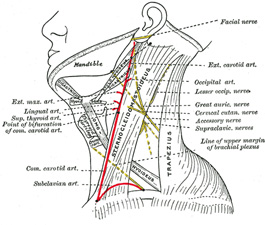 |
FIG. 1210– Side of neck, showing chief surface markings. (See enlarged image) |
| |
| |
| Muscles.—The posterior belly of Digastricus is marked out by a line from the tip of the mastoid process to the junction of the greater cornu and body of the hyoid bone; a line from this latter point to a point just lateral to the symphysis menti indicates the position of the anterior belly. The line of Omohyoideus begins at the lower border of the hyoid bone, curves downward and lateralward to cross Sternocleidomastoideus at the junction of its middle and lower thirds, i. e., opposite the cricoid cartilage, and then runs more horizontally to the acromial end of the clavicle. | 38 |
| |
| Arteries.—The position of the common carotid artery in the neck is indicated by a line drawn from the upper part of the sternal end of the clavicle to a point midway between the tip of the mastoid process and the angle of the mandible. From the clavicle to the upper border of the thyroid cartilage this line overlies the common carotid artery, beyond this it is over the external carotid. The external carotid artery may otherwise be marked out by the upper part of a line from the side of the cricoid cartilage to the front of the external acoustic meatus, arching the line slightly forward. | 39 |
| The points of origin of the main branches of the external carotid in the neck are all related to the tip of the greater cornu of the hyoid bone as follows: (1) the superior thyroid, immediately below it; (2) the lingual, on a level with it; (3) the facial, and (4) the occipital a little above and behind it. | 40 |
| The subclavian artery is indicated on the surface by a curved line, convex upward, from the sternoclavicular articulation to the middle of the clavicle. The highest point of the convexity is from 1 to 3 cm. above the clavicle. | 41 |
| |
| Veins.—The surface marking for the internal jugular vein is slightly lateral and parallel to that for the common carotid artery. The position of the external jugular vein is marked out by a line from the angle of the mandible to the middle of the clavicle. A point on this line about 4 cm. above the clavicle indicates the spot where the vein pierces the deep fascia. The line of the anterior jugular vein begins close to the symphysis menti, runs downward parallel with and a little to one side of the middle line and, at a variable distance above the jugular notch, turns lateralward to the external jugular. | 42 |
| |
| Nerves.—The facial nerve at its exit from the stylomastoid foramen is situated about 2.5 cm. from the surface, opposite the middle of the anterior border of the mastoid process; a horizontal line from this point to the ramus of the mandible overlies the stem of the nerve. To mark the site of the accessory nerve a line is drawn from the angle of the mandible to a point on the anterior border of Sternocleidomastoideus about 3 to 4 cm. below the apex of the mastoid process, or to the midpoint of the posterior border of the muscle; the line is continued across the posterior triangle to Trapezius. | 43 |
| The cutaneous branches of the cervical plexus as they emerge from the posterior border of Sternocleidomastoideus may be indicated as follows: the lesser occipital begins immediately above the midpoint of the border and runs along the border to the scalp; the great auricular and cervical cutaneous both start from the middle of the border, the former running upward toward the lobule of the auricula, the latter crossing Sternocleidomastoideus at right angles to its long axis; the supraclavicular nerves emerge from immediately below the middle of the posterior border and run down over the clavicle. The phrenic nerve begins at the level of the middle of the thyroid cartilage and runs behind the clavicle about midway between the anterior and posterior borders of Sternocleidomastoideus. | 44 |
| The upper border of the brachial plexus is indicated by a line from the side of the cricoid cartilage to the middle of the clavicle. | 45 |
| |
| Submaxillary Gland.—On either side of the neck the superficial portion of the submaxillary gland, as it lies partly under cover of the mandible, can be palpated. | 46 |