(Ossa Cranii) & (Os Occipitale).
The occipital bone (Figs. 129, 130), situated at the back and lower part of the cranium, is trapezoid in shape and curved on itself. It is pierced by a large oval aperture, the foramen magnum, through which the cranial cavity communicates with the vertebral canal. | 1 |
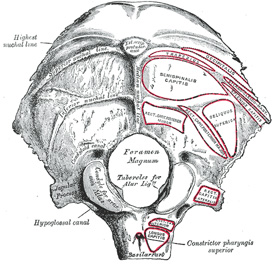 |
FIG. 129– Occipital bone. Outer surface. (See enlarged image) |
| |
| The curved, expanded plate behind the foramen magnum is named the squama; the thick, somewhat quadrilateral piece in front of the foramen is called the basilar part, whilst on either side of the foramen is the lateral portion. | 2 |
| |
| The Squama (squama occipitalis).—The squama, situated above and behind the foramen magnum, is curved from above downward and from side to side. | 3 |
| |
| Surfaces.—The external surface is convex and presents midway between the summit of the bone and the foramen magnum a prominence, the external occipital protuberance. Extending lateralward from this on either side are two curved lines, one a little above the other. The upper, often faintly marked, is named the highest nuchal line, and to it the galea aponeurotica is attached. The lower is termed the superior nuchal line. That part of the squama which lies above the highest nuchal lines is named the planum occipitale, and is covered by the Occipitalis muscle; that below, termed the planum nuchale, is rough and irregular for the attachment of several muscles. From the external occipital protuberance a ridge or crest, the median nuchal line, often faintly marked, descends to the foramen magnum, and affords attachment to the ligamentum nuchæ; running from the middle of this line across either half of the nuchal plane is the inferior nuchal line. Several muscles are attached to the outer surface of the squama, thus: the superior nuchal line gives origin to the Occipitalis and Trapezius, and insertion to the Sternocleidomastoideus and Splenius capitis: into the surface between the superior and inferior nuchal lines the Semispinalis capitis and the Obliquus capitis superior are inserted, while the inferior nuchal line and the area below it receive the insertions of the Recti capitis posteriores major and minor. The posterior atlantoöccipital membrane is attached around the postero-lateral part of the foramen magnum, just outside the margin of the foramen. | 4 |
 |
FIG. 130– Occipita bone. Inner surface. (See enlarged image) |
| |
| The internal surface is deeply concave and divided into four fossæ by a cruciate eminence. The upper two fossæ are triangular and lodge the occipital lobes of the cerebrum; the lower two are quadrilateral and accommodate the hemispheres of the cerebellum. At the point of intersection of the four divisions of the cruciate eminence is the internal occipital protuberance. From this protuberance the upper division of the cruciate eminence runs to the superior angle of the bone, and on one side of it (generally the right) is a deep groove, the sagittal sulcus, which lodges the hinder part of the superior sagittal sinus; to the margins of this sulcus the falx cerebri is attached. The lower division of the cruciate eminence is prominent, and is named the internal occipital crest; it bifurcates near the foramen magnum and gives attachment to the falx cerebelli; in the attached margin of this falx is the occipital sinus, which is sometimes duplicated. In the upper part of the internal occipital crest, a small depression is sometimes distinguishable; it is termed the vermian fossa since it is occupied by part of the vermis of the cerebellum. Transverse grooves, one on either side, extend from the internal occipital protuberance to the lateral angles of the bone; those grooves accommodate the transverse sinuses, and their prominent margins give attachment to the tentorium cerebelli. The groove on the right side is usually larger than that on the left, and is continuous with that for the superior sagittal sinus. Exceptions to this condition are, however, not infrequent; the left may be larger than the right or the two may be almost equal in size. The angle of union of the superior sagittal and transverse sinuses is named the confluence of the sinuses (torcular Herophili 25), and its position is indicated by a depression situated on one or other side of the protuberance. | 5 |
| |
| Lateral Parts (pars lateralis).—The lateral parts are situated at the sides of the foramen magnum; on their under surfaces are the condyles for articulation with the superior facets of the atlas. The condyles are oval or reniform in shape, and their anterior extremities, directed forward and medialward, are closer together than their posterior, and encroach on the basilar portion of the bone; the posterior extremities extend back to the level of the middle of the foramen magnum. The articular surfaces of the condyles are convex from before backward and from side to side, and look downward and lateralward. To their margins are attached the capsules of the atlantoöccipital articulations, and on the medial side of each is a rough impression or tubercle for the alar ligament. At the base of either condyle the bone is tunnelled by a short canal, the hypoglossal canal (anterior condyloid foramen). This begins on the cranial surface of the bone immediately above the foramen magnum, and is directed lateralward and forward above the condyle. It may be partially or completely divided into two by a spicule of bone; it gives exit to the hypoglossal or twelfth cerebral nerve, and entrance to a meningeal branch of the ascending pharyngeal artery. Behind either condyle is a depression, the condyloid fossa, which receives the posterior margin of the superior facet of the atlas when the head is bent backward; the floor of this fossa is sometimes perforated by the condyloid canal, through which an emissary vein passes from the transverse sinus. Extending lateralward from the posterior half of the condyle is a quadrilateral plate of bone, the jugular process, excavated in front by the jugular notch, which, in the articulated skull, forms the posterior part of the jugular foramen. The jugular notch may be divided into two by a bony spicule, the intrajugular process, which projects lateralward above the hypoglossal canal. The under surface of the jugular process is rough, and gives attachment to the Rectus capitis lateralis muscle and the lateral atlantoöccipital ligament; from this surface an eminence, the paramastoid process, sometimes projects downward, and may be of sufficient length to reach, and articulate with, the transverse process of the atlas. Laterally the jugular process presents a rough quadrilateral or triangular area which is joined to the jugular surface of the temporal bone by a plate of cartilage; after the age of twenty-five this plate tends to ossify. | 6 |
| The upper surface of the lateral part presents an oval eminence, the jugular tubercle, which overlies the hypoglossal canal and is sometimes crossed by an oblique groove for the glossopharyngeal, vagus, and accessory nerves. On the upper surface of the jugular process is a deep groove which curves medialward and forward and is continuous with the jugular notch. This groove lodges the terminal part of the transverse sinus, and opening into it, close to its medial margin, is the orifice of the condyloid canal. | 7 |
| |
| Basilar Part (pars basilaris).—The basilar part extends forward and upward from the foramen magnum, and presents in front an area more or less quadrilateral in outline. In the young skull this area is rough and uneven, and is joined to the body of the sphenoid by a plate of cartilage. By the twenty-fifth year this cartilaginous plate is ossified, and the occipital and sphenoid form a continuous bone. | 8 |
| |
| Surfaces.—On its lower surface, about 1 cm. in front of the foramen magnum, is the pharyngeal tubercle which gives attachment to the fibrous raphé of the pharynx. On either side of the middle line the Longus capitis and Rectus capitis anterior are inserted, and immediately in front of the foramen magnum the anterior atlantoöccipital membrane is attached. | 9 |
| The upper surface presents a broad, shallow groove which inclines upward and forward from the foramen magnum; it supports the medulla oblongata, and near the margin of the foramen magnum gives attachment to the membrana tectoria. On the lateral margins of this surface are faint grooves for the inferior petrosal sinuses. | 10 |
| |
| Foramen Magnum.—The foramen magnum is a large oval aperture with its long diameter antero-posterior; it is wider behind than in front where it is encroached upon by the condyles. It transmits the medulla oblongata and its membranes, the accessory nerves, the vertebral arteries, the anterior and posterior spinal arteries, and the membrana tectoria and alar ligaments. | 11 |
| |
| Angles.—The superior angle of the occipital bone articulates with the occipital angles of the parietal bones and, in the fetal skull, corresponds in position with the posterior fontanelle. The inferior angle is fused with the body of the sphenoid. The lateral angles are situated at the extremities of the grooves for the transverse sinuses: each is received into the interval between the mastoid angle of the parietal and the mastoid part of the temporal. | 12 |
| |
| Borders.—The superior borders extend from the superior to the lateral angles: they are deeply serrated for articulation with the occipital borders of the parietals, and form by this union the lambdoidal suture. The inferior borders extend from the lateral angles to the inferior angle; the upper half of each articulates with the mastoid portion of the corresponding temporal, the lower half with the petrous part of the same bone. These two portions of the inferior border are separated from one another by the jugular process, the notch on the anterior surface of which forms the posterior part of the jugular foramen. | 13 |
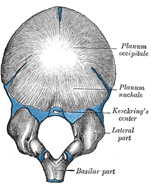 |
FIG. 131– Occipital bone at birth. (See enlarged image) |
| |
| |
| Structure.—The occipital, like the other cranial the outer and inner tables, between which is the cancellous tissue or diploë; the bone is especially thick at the ridges, protuberances, condyles, and anterior part of the basilar part; in the inferior fossæ it is thin, semitransparent, and destitute of diploë. | 14 |
| |
| Ossification (Fig. 131).—The planum occipitale of the squama is developed in membrane, and may remain separate throughout life when it constitutes the interparietal bone; the rest of the bone is developed in cartilage. The number of nuclei for the planum occipitale is usually given as four, two appearing near the middle line about the second month, and two some little distance from the middle line about the third month of fetal life. The planum nuchale of the squama is ossified from two centers, which appear about the seventh week of fetal life and soon unite to form a single piece. Union of the upper and lower portions of the squama takes place in the third month of fetal life. An occasional center (Kerckring) appears in the posterior margin of the foramen magnum during the fifth month; this forms a separate ossicle (sometimes double) which unites with the rest of the squama before birth. Each of the lateral parts begins to ossify from a single center during the eighth week of fetal life. The basilar portion is ossified from two centers, one in front of the other; these appear about the sixth week of fetal life and rapidly coalesce. Mall 26 states that the planum occipitale is ossified from two centers and the basilar portion from one. About the fourth year the squama and the two lateral portions unite, and about the sixth year the bone consists of a single piece. Between the eighteenth and twenty-fifth years the occipital and sphenoid become united, forming a single bone. | 15 |
| |
| Articulations.—The occipital articulates with six bones: the two parietals, the two temporals, the sphenoid, and the atlas. | 16 |