| The middle part of the fossa presents, in front, the chiasmatic groove and tuberculum sellæ; the chiasmatic groove ends on either side at the optic foramen, which transmits the optic nerve and ophthalmic artery to the orbital cavity. Behind the optic foramen the anterior clinoid process is directed backward and medialward and gives attachment to the tentorium cerebelli. Behind the tuberculum sellæ is a deep depression, the sella turcica, containing the fossa hypophyseos, which lodges the hypophysis, and presents on its anterior wall the middle clinoid processes. The sella turcica is bounded posteriorly by a quadrilateral plate of bone, the dorsum sellæ, the upper angles of which are surmounted by the posterior clinoid processes: these afford attachment to the tentorium cerebelli, and below each is a notch for the abducent nerve. On either side of the sella turcica is the carotid groove, which is broad, shallow, and curved somewhat like the italic letter f. It begins behind at the foramen lacerum, and ends on the medial side of the anterior clinoid process, where it is sometimes converted into a foramen (carotico-clinoid) by the union of the anterior with the middle clinoid process; posteriorly, it is bounded laterally by the lingula. This groove lodges the cavernous sinus and the internal carotid artery, the latter being surrounded by a plexus of sympathetic nerves. | 5 |
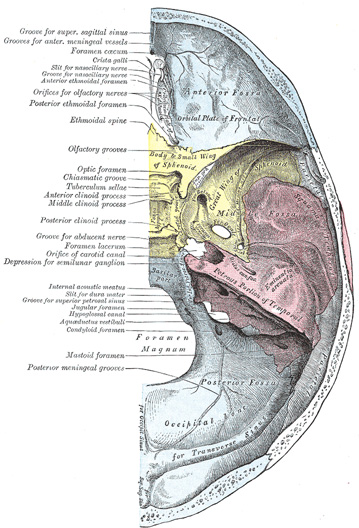 |
FIG. 193– Base of the skull. Upper surface. (See enlarged image) |
| |
| The lateral parts of the middle fossa are of considerable depth, and support the temporal lobes of the brain. They are marked by depressions for the brain convolutions and traversed by furrows for the anterior and posterior branches of the middle meningeal vessels. These furrows begin near the foramen spinosum, and the anterior runs forward and upward to the sphenoidal angle of the parietal, where it is sometimes converted into a bony canal; the posterior runs lateralward and backward across the temporal squama and passes on to the parietal near the middle of its lower border. The following apertures are also to be seen. In front is the superior orbital fissure, bounded above by the small wing, below, by the great wing, and medially, by the body of the sphenoid; it is usually completed laterally by the orbital plate of the frontal bone. It transmits to the orbital cavity the oculomotor, the trochlear, the ophthalmic division of the trigeminal, and the abducent nerves, some filaments from the cavernous plexus of the sympathetic, and the orbital branch of the middle meningeal artery; and from the orbital cavity a recurrent branch from the lacrimal artery to the dura mater, and the ophthalmic veins. Behind the medial end of the superior orbital fissure is the foramen rotundum, for the passage of the maxillary nerve. Behind and lateral to the foramen rotundum is the foramen ovale, which transmits the mandibular nerve, the accessory meningeal artery, and the lesser superficial petrosal nerve. 50 Medial to the foramen ovale is the foramen Vesalii, which varies in size in different individuals, and is often absent; when present, it opens below at the lateral side of the scaphoid fossa, and transmits a small vein. Lateral to the foramen ovale is the foramen spinosum, for the passage of the middle meningeal vessels, and a recurrent branch from the mandibular nerve. Medial to the foramen ovale is the foramen lacerum; in the fresh state the lower part of this aperture is filled up by a layer of fibrocartilage, while its upper and inner parts transmit the internal carotid artery surrounded by a plexus of sympathetic nerves. The nerve of the pterygoid canal and a meningeal branch from the ascending pharyngeal artery pierce the layer of fibrocartilage. On the anterior surface of the petrous portion of the temporal bone are seen the eminence caused by the projection of the superior semicircular canal; in front of and a little lateral to this a depression corresponding to the roof of the tympanic cavity; the groove leading to the hiatus of the facial canal, for the transmission of the greater superficial petrosal nerve and the petrosal branch of the middle meningeal artery; beneath it, the smaller groove, for the passage of the lesser superficial petrosal nerve; and, near the apex of the bone, the depression for the semilunar ganglion and the orifice of the carotid canal. | 6 |
| |
| The Posterior Fossa (fossa cranii posterior).—The posterior fossa is the largest and deepest of the three. It is formed by the dorsum sellæ and clivus of the sphenoid, the occipital, the petrous and mastoid portions of the temporals, and the mastoid angles of the parietal bones; it is crossed by the occipitomastoid and the parietomastoid sutures, and lodges the cerebellum, pons, and medulla oblongata. It is separated from the middle fossa in and near the median line by the dorsum sellæ of the sphenoid and on either side by the superior angle of the petrous portion of the temporal bone. This angle gives attachment to the tentorum cerebelli, is grooved for the superior petrosal sinus, and presents at its medial end a notch upon which the trigeminal nerve rests. The fossa is limited behind by the grooves for the transverse sinuses. In its center is the foramen magnum, on either side of which is a rough tubercle for the attachment of the alar ligaments; a little above this tubercle is the canal, which transmits the hypoglossal nerve and a meningeal branch from the ascending pharyngeal artery. In front of the foramen magnum the basilar portion of the occipital and the posterior part of the body of the sphenoid form a grooved surface which supports the medulla oblongata and pons; in the young skull these bones are joined by a synchondrosis. This grooved surface is separated on either side from the petrous portion of the temporal by the petro-occipital fissure, which is occupied in the fresh state by a plate of cartilage; the fissure is continuous behind with the jugular foramen, and its margins are grooved for the inferior petrosal sinus. The jugular foramen is situated between the lateral part of the occipital and the petrous part of the temporal. The anterior portion of this foramen transmits the inferior petrosal sinus; the posterior portion, the transverse sinus and some meningeal branches from the occipital and ascending pharyngeal arteries; and the intermediate portion, the glossopharyngeal, vagus, and accessory nerves. Above the jugular foramen is the internal acoustic meatus, for the facial and acoustic nerves and internal auditory artery; behind and lateral to this is the slit-like opening leading into the aquæductus vestibuli, which lodges the ductus endolymphaticus; while between these, and near the superior angle of the petrous portion, is a small triangular depression, the remains of the fossa subarcuata, which lodges a process of the dura mater and occasionally transmits a small vein. Behind the foramen magnum are the inferior occipital fossæ, which support the hemispheres of the cerebellum, separated from one another by the internal occipital crest, which serves for the attachment of the falx cerebelli, and lodges the occipital sinus. The posterior fossæ are surmounted by the deep grooves for the transverse sinuses. Each of these channels, in its passage to the jugular foramen, grooves the occipital, the mastoid angle of the parietal, the mastoid portion of the temporal, and the jugular process of the occipital, and ends at the back part of the jugular foramen. Where this sinus grooves the mastoid portion of the temporal, the orifice of the mastoid foramen may be seen; and, just previous to its termination, the condyloid canal opens into it; neither opening is constant. | 7 |
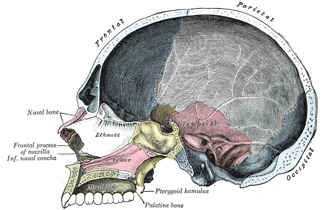 |
FIG. 194– Sagittal section of skull. (See enlarged image) |
| |
| |
| The Nasal Cavity (cavum nasi; nasal fossa).—The nasal cavities are two irregular spaces, situated one on either side of the middle line of the face, extending from the base of the cranium to the roof of the mouth, and separated from each other by a thin vertical septum. They open on the face through the pear-shaped anterior nasal aperture, and their posterior openings or choanæ communicate, in the fresh state, with the nasal part of the pharynx. They are much narrower above than below, and in the middle than at their anterior or posterior openings: their depth, which is considerable, is greatest in the middle. They communicate with the frontal, ethmoidal, sphenoidal, and maxillary sinuses. Each cavity is bounded by a roof, a floor, a medial and a lateral wall. | 8 |
| The roof (Figs. 195, 196) is horizontal in its central part, but slopes downward in front and behind; it is formed in front by the nasal bone and the spine of the frontal; in the middle, by the cribriform plate of the ethmoid; and behind, by the body of the sphenoid, the sphenoidal concha, the ala of the vomer and the sphenoidal process of the palatine bone. In the cribriform plate of the ethmoid are the foramina for the olfactory nerves, and on the posterior part of the roof is the opening into the sphenoidal sinus. | 9 |
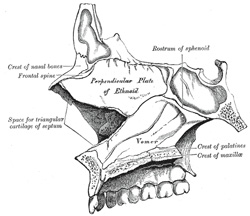 |
FIG. 195– Medial wall of left nasal fossa. (See enlarged image) |
| |
| The floor is flattened from before backward and concave from side to side. It is formed by the palatine process of the maxilla and the horizontal part of the palatine bone; near its anterior end is the opening of the incisive canal. | 10 |
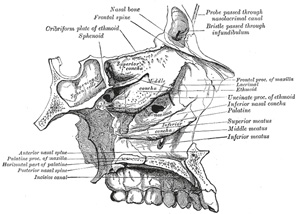 |
FIG. 196– Roof, floor, and lateral wall of left nasal cavity. (See enlarged image) |
| |
| The medial wall (septum nasi) (Fig. 195), is frequently deflected to one or other side, more often to the left than to the right. It is formed, in front, by the crest of the nasal bones and frontal spine; in the middle, by the perpendicular plate of the ethmoid; behind, by the vomer and the rostrum of the sphenoid; below, by the crest of the maxillæ and palatine bones. It presents, in front, a large, triangular notch, which receives the cartilage of the septum; and behind, the free edge of the vomer. Its surface is marked by numerous furrows for vessels and nerves and by the grooves for the nasopalatine nerve, and is traversed by sutures connecting the bones of which it is formed. | 11 |
| The lateral wall (Fig. 196) is formed, in front, by the frontal process of the maxilla and by the lacrimal bone; in the middle, by the ethmoid, maxilla, and inferior nasal concha; behind, by the vertical plate of the palatine bone, and the medial pterygoid plate of the sphenoid. On this wall are three irregular anteroposterior passages, termed the superior, middle, and inferior meatuses of the nose. The superior meatus, the smallest of the three, occupies the middle third of the lateral wall. It lies between the superior and middle nasal conchæ; the sphenopalatine foramen opens into it behind, and the posterior ethmoidal cells in front. The sphenoidal sinus opens into a recess, the sphenoethmoidal recess, which is placed above and behind the superior concha. The middle meatus is situated between the middle and inferior conchæ, and extends from the anterior to the posterior end of the latter. The lateral wall of this meatus can be satisfactorily studied only after the removal of the middle concha. On it is a curved fissure, the hiatus semilunaris, limited below by the edge of the uncinate process of the ethmoid and above by an elevation named the bulla ethmoidalis; the middle ethmoidal cells are contained within this bulla and open on or near to it. Through the hiatus semilunaris the meatus communicates with a curved passage termed the infundibulum, which communicates in front with the anterior ethmoidal cells and in rather more than fifty per cent. of skulls is continued upward as the frontonasal duct into the frontal air-sinus; when this continuity fails, the frontonasal duct opens directly into the anterior part of the meatus. Below the bulla ethmoidalis and hidden by the uncinate process of the ethmoid is the opening of the maxillary sinus (ostium maxillare); an accessory opening is frequently present above the posterior part of the inferior nasal concha. The inferior meatus, the largest of the three, is the space between the inferior concha and the floor of the nasal cavity. It extends almost the entire length of the lateral wall of the nose, is broader in front than behind, and presents anteriorly the lower orifice of the nasolacrimal canal. | 12 |
| The Anterior Nasal Aperture (Fig. 181) is a heart-shaped or pyriform opening, whose long axis is vertical, and narrow end upward; in the recent state it is much contracted by the lateral and alar cartilages of the nose. It is bounded above by the inferior borders of the nasal bones; laterally by the thin, sharp margins which separate the anterior from the nasal surfaces of the maxillæ; and below by the same borders, where they curve medialward to join each other at the anterior nasal spine. | 13 |
| The choanæ are each bounded above by the under surface of the body of the sphenoid and ala of the vomer; below, by the posterior border of the horizontal part of the palatine bone; laterally, by the medial pterygoid plate; they are separated from each other by the posterior border of the vomer. | 14 |
| |
| Differences in the Skull Due to AgeAt birth the skull is large in proportion to the other parts of the skeleton, but its facial portion is small, and equals only about one-eighth of the bulk of the cranium as compared with one-half in the adult. The frontal and parietal eminences are prominent, and the greatest width of the skull is at the level of the latter; on the other hand, the glabella, superciliary arches, and mastoid processes are not developed. Ossification of the skull bones is not completed, and many of them, e. g., the occipital, temporals, sphenoid, frontal, and mandible, consist of more than one piece. Unossified membranous intervals, termed fontanelles, are seen at the angles of the parietal bones; these fontanelles are six in number: two, an anterior and a posterior, are situated in the middle line, and two, an antero-lateral and a postero-lateral, on either side. | 15 |
| The anterior or bregmatic fontanelle (Fig. 197) is the largest, and is placed at the junction of the sagittal, coronal, and frontal sutures; it is lozenge-shaped, and measures about 4 cm. in its antero-posterior and 2.5 cm. in its transverse diameter. The posterior fontanelle is triangular in form and is situated at the junction of the sagittal and lambdoidal sutures. The lateral fontanelles (Fig. 198) are small, irregular in shape, and correspond respectively with the sphenoidal and mastoid angles of the parietal bones. An additional fontanelle is sometimes seen in the sagittal suture at the region of the obelion. The fontanelles are usually closed by the growth and extension of the bones which surround them, but sometimes they are the sites of separate ossific centers which develop into sutural bones. The posterior and lateral fontanelles are obliterated within a month or two after birth, but the anterior is not completely closed until about the middle of the second year. | 16 |
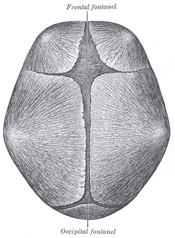 |
FIG. 197– Skull at birth, showing frontal and occipital fonticuli. (See enlarged image) |
| |
| The smallness of the face at birth is mainly accounted for by the rudimentary condition of the maxillæ and mandible, the non-eruption of the teeth, and the small size of the maxillary air sinuses and nasal cavities. At birth the nasal cavities lie almost entirely between the orbits, and the lower border of the anterior nasal aperture is only a little below the level of the orbital floor. With the eruption of the deciduous teeth there is an enlargement of the face and jaws, and these changes are still more marked after the second dentition. | 17 |
| The skull grows rapidly from birth to the seventh year, by which time the foramen magnum and petrous parts of the temporals have reached their full size and the orbital cavities are only a little smaller than those of the adult. Growth is slow from the seventh year until the approach of puberty, when a second period of activity occurs: this results in an increase in all directions, but it is especially marked in the frontal and facial regions, where it is associated with the development of the air sinuses. | 18 |
| Obliteration of the sutures of the vault of the skull takes place as age advances. This process may commence between the ages of thirty and forty, and is first seen on the inner surface, and some ten years later on the outer surface of the skull. The dates given are, however, only approximate, as it is impossible to state with anything like accuracy the time at which the sutures are closed. Obliteration usually occurs first in the posterior part of the sagittal suture, next in the coronal, and then in the lambdoidal. | 19 |
| In old age the skull generally becomes thinner and lighter, but in a small proportion of cases it increases in thickness and weight, owing to an hypertrophy of the inner table. The most striking feature of the old skull is the diminution in the size of the maxillæ and mandible consequent on the loss of the teeth and the absorption of the alveolar processes. This is associated with a marked reduction in the vertical measurement of the face and with an alteration in the angles of the mandible. | 20 |
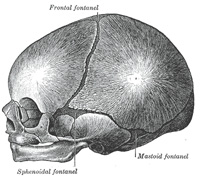 |
FIG. 198– Skull at birth, showing sphenoidal and mastoid fonticuli. (See enlarged image) |
| |
| |
| Sexual Differences in the SkullUntil the age of puberty there is little difference between the skull of the female and that of the male. The skull of an adult female is, as a rule, lighter and smaller, and its cranial capacity about 10 per cent. less, than that of the male. Its walls are thinner and its muscular ridges less strongly marked; the glabella, superciliary arches, and mastoid processes are less prominent, and the corresponding air sinuses are small or rudimentary. The upper margin of the orbit is sharp, the forehead vertical, the frontal and parietal eminences prominent, and the vault somewhat flattened. The contour of the face is more rounded, the facial bones are smoother, and the maxillæ and mandible and their contained teeth smaller. From what has been said it will be seen that more of the infantile characteristics are retained in the skull of the adult female than in that of the adult male. A well-marked male or female skull can easily be recognized as such, but in some cases the respective characteristics are so indistinct that the determination of the sex may be difficult or impossible. | 21 |
| |
| CraniologySkulls vary in size and shape, and the term craniology is applied to the study of these variations. The capacity of the cranial cavity constitutes a good index of the size of the brain which it contained, and is most conveniently arrived at by filling the cavity with shot and measuring the contents in a graduated vessel. Skulls may be classified according to their capacities as follows: | 22 |
| 1. Microcephalic, with a capacity of less than 1350 c.cm.—e.g., those of native Australians and Andaman Islanders. | 23 |
| 2. Mesocephalic, with a capacity of from 1350 c.cm. to 1450 c.cm.—e.g., those of African negroes and Chinese. | 24 |
| 3. Megacephalic, with a capacity of over 1450 c.cm.—e.g., those of Europeans, Japanese, and Eskimos. | 25 |
| In comparing the shape of one skull with that of another it is necessary to adopt some definite position in which the skulls should be placed during the process of examination. They should be so placed that a line carried through the lower margin of the orbit and upper margin of the external acoustic meatus is in the horizontal plane. The normæ of one skull can then be compared with those of another, and the differences in contour and surface form noted. Further, it is necessary that the various linear measurements used to determine the shape of the skull should be made between definite and easily localized points on its surface. The principal points may be divided into two groups: (1) those in the median plane, and (2) those on either side of it. | 26 |
| The Points in the Median Plane are the: | 27 |
| Mental Point. The most prominent point of the chin. | 28 |
| Alveolar Point or Prosthion. The central point of the anterior margin of the upper alveolar arch. | 29 |
| Subnasal Point. The middle of the lower border of the anterior nasal aperture, at the base of the anterior nasal spine. | 30 |
| Nasion. The central point of the frontonasal suture. | 31 |
| Glabella. The point in the middle line at the level of the superciliary arches. | 32 |
| Ophryon. The point in the middle line of the forehead at the level where the temporal lines most nearly approach each other. | 33 |
| Bregma. The meeting point of the coronal and sagittal sutures. | 34 |
| Obelion. A point in the sagittal suture on a level with the parietal foramina. | 35 |
| Lambda. The point of junction of the sagittal and lambdoidal sutures. | 36 |
| Occipital Point. The point in the middle line of the occipital bone farthest from the glabella. | 37 |
| Inion. The external occipital protuberance. | 38 |
| Opisthion. The mid-point of the posterior margin of the foramen magnum. | 39 |
| Basion. The mid-point of the anterior margin of the foramen magnum. | 40 |
| The Points on Either Side of the Median Plane are the: | 41 |
| Gonion. The outer margin of the angle of the mandible. | 42 |
| Dacryon. The point of union of the antero-superior angle of the lacrimal with the frontal bone and the frontal process of the maxilla. | 43 |
| Stephanion. The point where the temporal line intersects the coronal suture. | 44 |
| Pterion. The point where the great wing of the sphenoid joins the sphenoidal angle of the parietal. | 45 |
| Auricular Point. The center of the orifice of the external acoustic meatus. | 46 |
| Asterion. The point of meeting of the lambdoidal, mastoöccipital, and mastoparietal sutures. | 47 |
| The horizontal circumference of the cranium is measured in a plane passing through the glabella (Turner) or the ophryon (Flower) in front, and the occipital point behind; it averages about 50 cm. in the female and 52.5 cm. in the male. | 48 |
| The occipitofrontal or longitudinal arc is measured from the nasion over the middle line of the vertex to the opisthion: while the basinasal length is the distance between the basion and the nasion. These two measurements, plus the antero-posterior diameter of the foramen magnum, represent the vertical circumference of the cranium. | 49 |
| The length is measured from the glabella to the occipital point, while the breadth or greatest transverse diameter is usually found near the external acoustic meatus. The proportion of breadth to length (breadth X 100)/length is termed the cephalic index or index of breadth. | 50 |
| The height is usually measured from the basion to the bregma, and the proportion of height to length (height X 100)/length constitutes the vertical or height index. | 51 |
| In studying the face the principal points to be noticed are the proportion of its length and breadth, the shape of the orbits and of the anterior nasal aperture, and the degree of projection of the jaws. | 52 |
| The length of the face may be measured from the ophryon or nasion to the chin, or, if the mandible be wanting, to the alveolar point; while its width is represented by the distance between the zygomatic arches. By comparing the length with the width of the face, skulls may be divided into two groups; dolichofacial or leptoprosope (long faced) and brachyfacial or chemoprosope (short faced). | 53 |
The orbital index signifies the proportion which the orbital height bears to the orbital width, thus:
| orbital height X 100/orbital width |
| 54 |
The nasal index expresses the proportion which the width of the anterior nasal aperture bears to the height of the nose, the latter being measured from the nasion to the lower margin of the nasal aperture, thus:| nasal width X 100/nasal height |
| 55 |
The degree of projection of the jaws is determined by the gnathic or alveolar index, which represents the proportion between the basialveolar and basinasal lengths, thus:| basialveolar length X 100/basinasal length |
| 56 |
| The following table, modified from that given by Duckworth, 51 illustrates how these different indices may be utilized in the classification of skulls: | 57 |
| Index. |
Classification. |
Nomenclature. |
Examples. |
| 1. Cephalic |
Below 75 |
Dolichocephalic |
Kaffirs and Native Australians. |
|
Between 75 and 80 |
Mesaticephalic |
Europeans and Chinese. |
| Above 80 |
Brachycephalic |
Mongolians and Andamans. |
| 2. Orbital |
Below 84 |
Microseme |
Tasmanians and Native Australians. |
|
Between 84 and 89 |
Mesoseme |
Europeans. |
| Above 89 |
Megaseme |
Chinese and Polynesians. |
| 3. Nasal |
Below 48 |
Leptorhine |
Europeans. |
|
Between 48 and 53 |
Mesorhine |
Japanese and Chinese. |
| Above 53 |
Platyrhine |
Negroes and Native Australians. |
| 4. Gnathic |
Below 98 |
Orthognathous |
Europeans. |
|
Between 98 and 103 |
Mesognathous |
Chinese and Japanese. |
| Above 103 |
Prognathous |
Native Australians. |
|
| The chief function of the skull is to protect the brain, and therefore those portions of the skull which are most exposed to external violence are thicker than those which are shielded from injury by overlying muscles. Thus, the skull-cap is thick and dense, whereas the temporal squamæ being protected by the temporales muscles, and the inferior occipital fossæ, being shielded by the muscles at the back of the neck, are thin and fragile. Fracture of the skull is further prevented by its elasticity, its rounded shape, and its construction of a number of secondary elastic arches, each made up of a single bone. The manner in which vibrations are transmitted through the bones of the skull is also of importance as regards its protective mechanism, at all events as far as the base is concerned. In the vault, the bones being of a fairly equal thickness and density, vibrations are transmitted in a uniform manner in all directions, but in the base, owing to the varying thickness and density of the bones, this is not so; and therefore in this situation there are special buttresses which serve to carry the vibrations in certain definite directions. At the front of the skull, on either side, is the ridge which separates the anterior from the middle fossa of the base; and behind, the ridge or buttress which separates the middle from the posterior fossa; and if any violence is applied to the vault, the vibrations would be carried along these buttresses to the sella turcica, where they meet. This part has been termed the “center of resistance,” and here there is a special protective mechanism to guard the brain. The subarachnoid cavity at the base of the brain is dilated, and the cerebrospinal fluid which fills it acts as a water cushion to shield the brain from injury. In like manner, when violence is applied to the base of the skull, as in falls upon the feet, the vibrations are carried backward through the occipital crest, and forward through the basilar part of the occipital and body of the sphenoid to the vault of the skull. | 58 |
 |
FIG. 199– The premaxilla and its sutures. (After Albrecht.) (See enlarged image) |
| |
| In connection with the bones of the face a common malformation is cleft palate. The cleft usually starts posteriorly, and its most elementary form is a bifid uvula; or the cleft may extend through the soft palate; or the posterior part of the whole of the hard palate may be involved, the cleft extending as far forward as the incisive foramen. In the severest forms, the cleft extends through the alveolus and passes between the incisive or premaxillary bone and the rest of the maxilla; that is to say, between the lateral incisor and canine teeth. In some instances, the cleft runs between the central and lateral incisor teeth; and this has induced some anatomists to believe that the premaxillary bone is developed from two centers (Fig. 199) and not from one, as was stated on p. 163. The medial segment, bearing a central incisor, is called an endognathion; the lateral segment, bearing the lateral incisor, is called a mesognathion. The cleft may affect one or both sides; if the latter, the central part is frequently displaced forward and remains united to the septum of the nose, the deficiency in the alveolus being complicated with a cleft in the lip (hare-lip). On examining a cleft palate in which the alveolus is not implicated, the cleft will generally appear to be in the median line, but occasionally is unilateral and in some cases bilateral. To understand this it must be borne in mind that three processes are concerned in the formation of the palate—the palatine processes of the two maxillæ, which grow in horizontally and unite in the middle line, and the ethmovomerine process, which grows downward from the base of the skull and frontonasal process to unite with the palatine processes in the middle line. In those cases where the palatine processes fail to unite with each other and with the medial process, the cleft of the palate is median; where one palatine process unites with the medial septum, the other failing to do so, the cleft in the palate is unilateral. In some cases where the palatine processes fail to meet in the middle, the ethmovomerine process grows downward between them and thus produces a bilateral cleft. Occasionally there may be a hole in the middle line of the hard palate, the anterior part of the hard and the soft palate being perfect; this is rare, because, as a rule, the union of the various processes progresses from before backward, and therefore the posterior part of the palate is more frequently defective than the anterior. | 59 |