(Ventriculus; Gaster)
The stomach is the most dilated part of the digestive tube, and is situated between the end of the esophagus and the beginning of the small intestine. It lies in the epigastric, umbilical, and left hypochondriac regions of the abdomen, and occupies a recess bounded by the upper abdominal viscera, and completed in front and on the left side by the anterior abdominal wall and the diaphragm. | 1 |
| The shape and position of the stomach are so greatly modified by changes within itself and in the surrounding viscera that no one form can be described as typical. The chief modifications are determined by (1) the amount of the stomach contents, (2) the stage which the digestive process has reached, (3) the degree of development of the gastric musculature, and (4) the condition of the adjacent intestines. It is, however, possible by comparing a series of stomachs to determine certain markings more or less common to all (Figs. 1046, 1047, 1048, 1049). | 2 |
| The stomach presents two openings, two borders or curvatures, and two surfaces. | 3 |
| |
| Openings.—The opening by which the esophagus communicates with the stomach is known as the cardiac orifice, and is situated on the left of the middle line at the level of the tenth thoracic vertebra. The short abdominal portion of the esophagus (antrum cardiacum) is conical in shape and curved sharply to the left, the base of the cone being continuous with the cardiac orifice of the stomach. The right margin of the esophagus is continuous with the lesser curvature of the stomach, while the left margin joins the greater curvature at an acute angle, termed the incisura cardiaca. | 4 |
| The pyloric orifice communicates with the duodenum, and its position is usually indicated on the surface of the stomach by a circular groove, the duodenopyloric constriction. This orifice lies to the right of the middle line at the level of the upper border of the first lumbar vertebra. | 5 |
| |
| Curvatures.—The lesser curvature (curvatura ventriculi minor), extending between the cardiac and pyloric orifices, forms the right or posterior border of the stomach. It descends as a continuation of the right margin of the esophagus in front of the fibers of the right crus of the diaphragm, and then, turning to the right, it crosses the first lumbar vertebra and ends at the pylorus. Nearer its pyloric than its cardiac end is a well-marked notch, the incisura angularis, which varies somewhat in position with the state of distension of the viscus; it serves to separate the stomach into a right and a left portion. The lesser curvature gives attachment to the two layers of the hepatogastric ligament, and between these two layers are the left gastric artery and the right gastric branch of the hepatic artery. | 6 |
| The greater curvature (curvatura ventriculi major) is directed mainly forward, and is four or five times as long as the lesser curvature. Starting from the cardiac orifice at the incisura cardiaca, it forms an arch backward, upward, and to the left; the highest point of the convexity is on a level with the sixth left costal cartilage. From this level it may be followed downward and forward, with a slight convexity to the left as low as the cartilage of the ninth rib; it then turns to the right, to the end of the pylorus. Directly opposite the incisura angularis of the lesser curvature the greater curvature presents a dilatation, which is the left extremity of the pyloric part; this dilatation is limited on the right by a slight groove, the sulcus intermedius, which is about 2.5 cm, from the duodenopyloric constriction. The portion between the sulcus intermedius and the duodenopyloric constriction is termed the pyloric antrum. At its commencement the greater curvature is covered by peritoneum continuous with that covering the front of the organ. The left part of the curvature gives attachment to the gastrolienal ligament, while to its anterior portion are attached the two layers of the greater omentum, separated from each other by the gastroepiploic vessels. | 7 |
| |
| Surfaces.—When the stomach is in the contracted condition, its surfaces are directed upward and downward respectively, but when the viscus is distended they are directed forward, and backward. They may therefore be described as anterosuperior and postero-inferior. | 8 |
| |
| Antero-superior Surface.—The left half of this surface is in contact with the diaphragm, which separates it from the base of the left lung, the pericardium, and the seventh, eighth, and ninth ribs, and intercostal spaces of the left side. The right half is in relation with the left and quadrate lobes of the liver and with the anterior abdominal wall. When the stomach is empty, the transverse colon may lie on the front part of this surface. The whole surface is covered by peritoneum. | 9 |
| The Postero-inferior Surface is in relation with the diaphragm, the spleen, the left suprarenal gland, the upper part of the front of the left kidney, the anterior surface of the pancreas, the left colic flexure, and the upper layer of the transverse mesocolon. These structures form a shallow bed, the stomach bed, on which the viscus rests. The transverse mesocolon separates the stomach from the duodenojejunal flexure and small intestine. The postero-inferior surface is covered by peritoneum, except over a small area close to the cardiac orifice; this area is limited by the lines of attachment of the gastrophrenic ligament, and lies in apposition with the diaphragm, and frequently with the upper portion of the left suprarenal gland. | 10 |
| |
| Component Parts of the Stomach.—A plane passing through the incisura angularis on the lesser curvature and the left limit of the opposed dilatation on the greater curvature divides the stomach into a left portion or body and a right or pyloric portion. The left portion of the body is known as the fundus, and is marked off from the remainder of the body by a plane passing horizontally through the cardiac orifice. The pyloric portion is divided by a plane through the sulcus intermedius at right angles to the long axis of this portion; the part to the right of this plane is the pyloric antrum (Fig. 1046). | 11 |
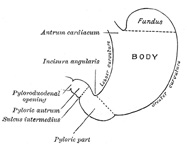 |
FIG. 1046– Outline of stomach, showing its anatomical landmarks. (See enlarged image) |
| |
 |
FIG. 1047– Diagram showing shape and position of empty stomach. Erect posture. (Hertz.) (See enlarged image) |
| |
| If the stomach be examined during the process of digestion it will be found divided by a muscular constriction into a large dilated left portion, and a narrow contracted tubular right portion. The constriction is in the body of the stomach, and does not follow any of the anatomical landmarks; indeed, it shifts gradually toward the left as digestion progresses, i. e., more of the body is gradually absorbed into the tubular part (Figs. 1047, 1048, 1049). | 12 |
 |
FIG. 1048– Diagram showing shape and position of moderately filled stomach. Erect posture. (Hertz.) (See enlarged image) |
| |
 |
FIG. 1049– Diagram showing shape and position of distended stomach. Erect posture. (Hertz.) (See enlarged image) |
| |
| |
| Position of the Stomach.—The position of the stomach varies with the posture, with the amount of the stomach contents and with the condition of the intestines on which it rests. In the erect posture the empty stomach is somewhat J-shaped; the part above the cardiac orifice is usually distended with gas; the pylorus descends to the level of the second lumbar vertebra and the most dependent part of the stomach is at the level of the umbilicus. Variation in the amount of its contents affects mainly the cardiac portion, the pyloric portion remaining in a more or less contracted condition during the process of digestion. As the stomach fills it tends to expand forward and downward in the direction of least resistance, but when this is interfered with by a distended condition of the colon or intestines the fundus presses upward on the liver and diaphragm and gives rise to the feelings of oppression and palpitation complained of in such cases. His 166 and Cunningham 167 have shown by hardening the viscera in situ that the contracted stomach has a sickle shape, the fundus looking directly backward. The surfaces are directed upward and downward, the upper surface having, however, a gradual downward slope to the right. The greater curvature is in front and at a slightly higher level than the lesser. | 13 |
| The position of the full stomach depends, as already indicated, on the state of the intestines; when these are empty the fundus expands vertically and also forward, the pylorus is displaced toward the right and the whole organ assumes an oblique position, so that its surfaces are directed more forward and backward. The lowest part of the stomach is at the pyloric vestibule, which reaches to the region of the umbilicus. Where the intestines interfere with the downward expansion of the fundus the stomach retains the horizontal position which is characteristic of the contracted viscus. | 14 |
| Examination of the stomach during life by x-rays has confirmed these findings, and has demonstrated that, in the erect posture, the full stomach usually presents a hook-like appearance, the long axis of the clinical fundus being directed downward, medialward, and forward toward the umbilicus, while the pyloric portion curves upward to the duodenopyloric junction. | 15 |
| |
| Interior of the Stomach.—When examined after death, the stomach is usually fixed at some temporary stage of the digestive process. A common form is that shown in Fig. 1050. If the viscus be laid open by a section through the plane of its two curvatures, it is seen to consist of two segments: (a) a large globular portion on the left and (b) a narrow tubular part on the right. These correspond to the clinical subdivisions of fundus and pyloric portions already described, and are separated by a constriction which indents the body and greater curvature, but does not involve the lesser curvature. To the left of the cardiac orifice is the incisura cardiaca: the projection of this notch into the cavity of the stomach increases as the organ distends, and has been supposed to act as a valve preventing regurgitation into the esophagus. In the pyloric portion are seen: (a) the elevation corresponding to the incisura angularis, and (b) the circular projection from the duodenopyloric constriction which forms the pyloric valve; the separation of the pyloric antrum from the rest of the pyloric part is scarcely indicated. | 16 |
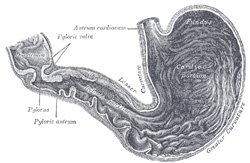 |
FIG. 1050– Interior of the stomach. (See enlarged image) |
| |
| The pyloric valve (valvula pylori) is formed by a reduplication of the mucous membrane of the stomach, covering a muscular ring composed of a thickened portion of the circular layer of the muscular coat. Some of the deeper longitudinal fibers turn in and interlace with the circular fibers of the valve. | 17 |
| |
| Structure.—The wall of the stomach consists of four coats: serous, muscular, areolar, and mucous, together with vessels and nerves. | 18 |
| The serous coat (tunica serosa) is derived from the peritoneum, and covers the entire surface of the organ, excepting along the greater and lesser curvatures at the points of attachment of the greater and lesser omenta; here the two layers of peritoneum leave a small triangular space, along which the nutrient vessels and nerves pass. On the posterior surface of the stomach, close to the cardiac orifice, there is also a small area uncovered by peritoneum, where the organ is in contact with the under surface of the diaphragm. | 19 |
| The muscular coat (tunica muscularis) (Figs. 1051, 1052) is situated immediately beneath the serous covering, with which it is closely connected. It consists of three sets of smooth muscle fibers: longitudinal, circular and oblique. | 20 |
| The longitudinal fibers (stratum longitudinale) are the most superficial, and are arranged in two sets. The first set consists of fibers continuous with the longitudinal fibers of the esophagus; they radiate in a stellate manner from the cardiac orifice and are practically all lost before the pyloric portion is reached. The second set commences on the body of the stomach and passes to the right, its fibers becoming more thickly distributed as they approach the pylorus. Some of the more superficial fibers of this set pass on to the duodenum, but the deeper fibers dip inward and interlace with the circular fibers of the pyloric valve. | 21 |
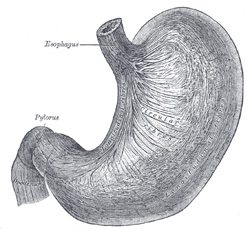 |
FIG. 1051– The longitudinal and circular muscular fibers of the stomach, viewed from above and in front. (Spalteholz.) (See enlarged image) |
| |
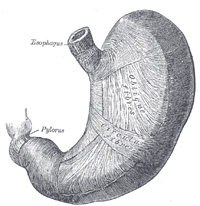 |
FIG. 1052– The oblique muscular fibers of the stomach, viewed from above and in front. (Spalteholz.) (See enlarged image) |
| |
| The circular fibers (stratum circulare) form a uniform layer over the whole extent of the stomach beneath the longitudinal fibers. At the pylorus they are most abundant, and are aggregated into a circular ring, which projects into the lumen, and forms, with the fold of mucous membrane covering its surface, the pyloric valve. They are continuous with the circular fibers of the esophagus, but are sharply marked off from the circular fibers of the duodenum. | 22 |
| The oblique fibers (fibræ obliquæ) internal to the circular layer, are limited chiefly to the cardiac end of the stomach, where they are disposed as a thick uniform layer, covering both surfaces, some passing obliquely from left to right, others from right to left, around the cardiac end. | 23 |
| The areolar or submucous coat (tela submucosa) consists of a loose, areolar tissue, connecting the mucous and muscular layers. | 24 |
| The mucous membrane (tunica mucosa) is thick and its surface is smooth, soft, and velvety. In the fresh state it is of a pinkish tinge at the pyloric end, and of a red or reddish-brown color over the rest of its surface. In infancy it is of a brighter hue, the vascular redness being more marked. It is thin at the cardiac extremity, but thicker toward the pylorus. During the contracted state of the organ it is thrown into numerous plaits or rugæ, which, for the most part, have a longitudinal direction, and are most marked toward the pyloric end of the stomach, and along the greater curvature (Fig. 1050). These folds are entirely obliterated when the organ becomes distended. | 25 |
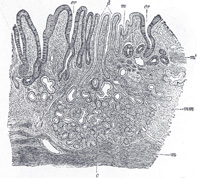 |
FIG. 1053– Section of mucous membrane of human stomach, near the cardiac orifice. (v. Ebner, after J. Schaffer.) X 45. c. Cardiac glands. d. Their ducts. cr. Gland similar to the intestinal glands, with goblet cells. mm. Mucous membrane. m. Muscularis mucosæ. m’. Muscular tissue within the mucous membrane. (See enlarged image) |
| |
| Structure of the Mucous Membrane.—When examined with a lens, the inner surface of the mucous membrane presents a peculiar honeycomb appearance from being covered with small shallow depressions or alveoli, of a polygonal or hexagonal form, which vary from 0.12 to 0.25 mm. in diameter. These are the ducts of the gastric glands, and at the bottom of each may be seen one or more minute orifices, the openings of the gland tubes. The surface of the mucous membrane is covered by a single layer of columnar epithelium with occasional goblet cells. This epithelium commences very abruptly at the cardiac orifice, where there is a sudden transition from the stratified epithelium of the esophagus. The epithelial lining of the gland ducts is of the same character and is continuous with the general epithelial lining of the stomach (Fig. 1055). | 26 |
| |
| The Gastric Glands.—The gastric glands are of three kinds: (a) pyloric, (b) cardiac, and (c) fundus or oxyntic glands. They are tubular in character, and are formed of a delicate basement membrane, consisting of flattened transparent endothelial cells lined by epithelium. The pyloric glands (Fig. 1054) are found in the pyloric portion of the stomach. They consist of two or three short closed tubes opening into a common duct or mouth. These tubes are wavy, and are about one-half the length of the duct. The duct is lined by columnar cells, continuous with the epithelium lining the surface of the mucous membrane of the stomach, the tubes by shorter and more cubical cell which are finely granular. The cardiac glands (Fig. 1053), few in number, occur close to the cardiac orifice. They are of two kinds: (1) simple tubular glands resembling those of the pyloric end of the stomach, but with short ducts; (2) compound racemose glands resembling the duodenal glands. The fundus glands (Fig. 1055) are found in the body and fundus of the stomach; they are simple tubes, two or more of which open into a single duct. The duct, however, in these glands is shorter than in the pyloric variety, sometimes not amounting to more than one-sixth of the whole length of the gland; it is lined throughout by columnar epithelium. The gland tubes are straight and parallel to each other. At the point where they open into the duct, which is termed the neck, the epithelium alters, and consists of short columnar or polyhedral, granular cells, which almost fill the tube, so that the lumen becomes suddenly constricted and is continued down as a very fine channel. They are known as the chief or central cells of the glands. Between these cells and the basement membrane, larger oval cells, which stain deeply with eosin, are found; these cells are studded throughout the tube at intervals, giving it a beaded or varicose appearance. These are known as the parietal or oxyntic cells, and they are connected with the lumen by fine channels which run into their substance. Between the glands the mucous membrane consists of a connective-tissue frame-work, with lymphoid tissue. In places, this later tissue, especially in early life, is collected into little masses, which to a certain extent resemble the solitary nodules of the intestine, and are termed the lenticular glands of the stomach. They are not, however, so distinctly circumscribed as the solitary nodules. Beneath the mucous membrane, and between it and the submucous coat, is a thin stratum of involuntary muscular fiber (muscularis mucosæ), which in some parts consists only of a single longitudinal layer; in others of two layers, an inner circular and an outer longitudinal. | 27 |
 |
FIG. 1054– A pyloric gland, from a section of the dog’s stomach. (Ebstein.) m. Mouth. n. Neck. tr. A deep portion of a tubule cut transversely. (See enlarged image) |
| |
 |
FIG. 1055– A fundus gland. A. Transverse section of gland. (See enlarged image) |
| |
| |
| Vessels and Nerves.—The arteries supplying the stomach are: the left gastric, the right gastric and right gastroepiploic branches of the hepatic, and the left gastroepiploic and short gastric branches of the lienal. They supply the muscular coat, ramify in the submucous coat, and are finally distributed to the mucous membrane. The arrangement of the vessels in the mucous membrane is somewhat peculiar. The arteries break up at the base of the gastric tubules into a plexus of fine capillaries which run upward between the tubules, anastomosing with each other, and ending in a plexus of larger capillaries, which surround the mouths of the tubes, and also form hexagonal meshes around the ducts. From these the veins arise, and pursue a straight course downward, between the tubules, to the submucous tissue; they end either in the lienal and superior mesenteric veins, or directly in the portal vein. The lymphatics are numerous: they consist of a superficial and a deep set, and pass to the lymph glands found along the two curvatures of the organ (page 706). The nerves are the terminal branches of the right and left vagi, the former being distributed upon the back, and the latter upon the front part of the organ. A great number of branches from the celiac plexus of the sympathetic are also distributed to it. Nerve plexuses are found in the submucous coat and between the layers of the muscular coat as in the intestine. From these plexuses fibrils are distributed to the muscular tissue and the mucous membrane. | 28 |