(Hepar)
The liver, the largest gland in the body, has both external and internal secretions, which are formed in the hepatic cells. Its external secretion, the bile, is collected after passing through the bile capillaries by the bile ducts, which join like the twigs and branches of a tree to form two large ducts that unite to form the hepatic duct. The bile is either carried to the gall-bladder by the cystic duct or poured directly into the duodenum by the common bile duct where it aids in digestion. The internal secretions are concerned with the metabolism of both nitrogenous and carbohydrate materials absorbed from the intestine and carried to the liver by the portal vein. The carbohydrates are stored in the hepatic cells in the form of glycogen which is secreted in the form of sugar directly into the blood stream. Some of the cells lining the blood capillaries of the liver are concerned in the destruction of red blood corpuscles. It is situated in the upper and right parts of the abdominal cavity, occupying almost the whole of the right hypochondrium, the greater part of the epigastrium, and not uncommonly extending into the left hypochondrium as far as the mammillary line. In the male it weighs from 1.4 to 1.6 kilogm., in the female from 1.2 to 1.4 kilogm. It is relatively much larger in the fetus than in the adult, constituting, in the former, about one-eighteenth, and in the latter about one thirty-sixth of the entire body weight. Its greatest transverse measurement is from 20 to 22.5 cm. Vertically, near its lateral or right surface, it measures about 15 to 17.5 cm., while its greatest antero-posterior diameter is on a level with the upper end of the right kidney, and is from 10 to 12.5 cm. Opposite the vertebral column its measurement from before backward is reduced to about 7.5 cm. Its consistence is that of a soft solid; it is friable, easily lacerated and highly vascular; its color is a dark reddish brown, and its specific gravity is 1.05. | 1 |
| To obtain a correct idea of its shape it must be hardened in situ, and it will then be seen to present the appearance of a wedge, the base of which is directed to the right and the thin edge toward the left. Symington describes its shape as that “of a right-angled triangular prism with the right angle rounded off.” | 2 |
| |
| Surfaces.—The liver possesses three surfaces, viz., superior, inferior and posterior. A sharp, well-defined margin divides the inferior from the superior in front; the other margins are rounded. The superior surface is attached to the diaphragm and anterior abdominal wall by a triangular or falciform fold of peritoneum, the falciform ligament, in the free margin of which is a rounded cord, the ligamentum teres (obliterated umbilical vein). The line of attachment of the falciform ligament divides the liver into two parts, termed the right and left lobes, the right being much the larger. The inferior and posterior surfaces are divided into four lobes by five fossæ, which are arranged in the form of the letter H. The left limb of the H marks on these surfaces the division of the liver into right and left lobes; it is known as the left sagittal fossa, and consists of two parts, viz., the fossa for the umbilical vein in front and the fossa for the ductus venosus behind. The right limb of the H is formed in front by the fossa for the gall-bladder, and behind by the fossa for the inferior vena cava; these two fossæ are separated from one another by a band of liver substance, termed the caudate process. The bar connecting the two limbs of the H is the porta (transverse fissure); in front of it is the quadrate lobe, behind it the caudate lobe. | 3 |
| The superior surface (facies superior) (Fig. 1085) comprises a part of both lobes, and, as a whole, is convex, and fits under the vault of the diaphragm which in front separates it on the right from the sixth to the tenth ribs and their cartilages, and on the left from the seventh and eighth costal cartilages. Its middle part lies behind the xiphoid process, and, in the angle between the diverging rib cartilage of opposite sides, is in contact with the abdominal wall. Behind this the diaphragm separates the liver from the lower part of the lungs and pleuræ, the heart and pericardium and the right costal arches from the seventh to the eleventh inclusive. It is completely covered by peritoneum except along the line of attachment of the falciform ligament. | 4 |
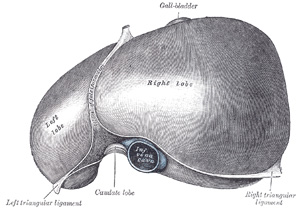 |
FIG. 1085– The superior surface of the liver. (From model by His.) (See enlarged image) |
| |
| The inferior surface (facies inferior; visceral surface) (Figs. 1086, 1087), is uneven, concave, directed downward, backward, and to the left, and is in relation with the stomach and duodenum, the right colic flexure, and the right kidney and suprarenal gland. The surface is almost completely invested by peritoneum; the only parts devoid of this covering are where the gall-bladder is attached to the liver, and at the porta hepatis where the two layers of the lesser omentum are separated from each other by the bloodvessels and ducts of the liver. The inferior surface of the left lobe presents behind and to the left the gastric impression, moulded over the antero-superior surface of the stomach, and to the right of this a rounded eminence, the tuber omentale, which fits into the concavity of the lesser curvature of the stomach and lies in front of the anterior layer of the lesser omentum. The under surface of the right lobe is divided into two unequal portions by the fossa for the gall-bladder; the portion to the left, the smaller of the two, is the quadrate lobe, and is in relation with the pyloric end of the stomach, the superior portion of the duodenum, and the transverse colon. The portion of the under surface of the right lobe to the right of the fossa for the gall-bladder presents two impressions, one situated behind the other, and separated by a ridge. The anterior of these two impressions, the colic impression, is shallow and is produced by the right colic flexure; the posterior, the renal impression, is deeper and is occupied by the upper part of the right kidney and lower part of the right suprarenal gland. Medial to the renal impression is a third and slightly marked impression, lying between it and the neck of the gall-bladder. This is caused by the descending portion of the duodenum, and is known as the duodenal impression. Just in front of the inferior vena cava is a narrow strip of liver tissue, the caudate process, which connects the right inferior angle of the caudate lobe to the under surface of the right lobe. It forms the upper boundary of the epiploic foramen of the peritoneum. | 5 |
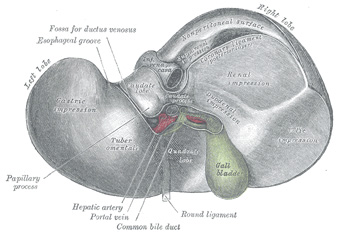 |
FIG. 1086– Inferior surface of the liver. (From model by His.) (See enlarged image) |
| |
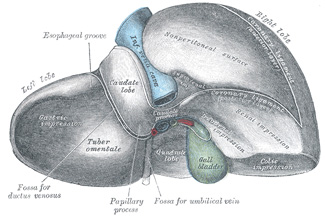 |
FIG. 1087– Posterior and inferior surfaces of the liver. (From model by His.) (See enlarged image) |
| |
| The posterior surface (facies posterior) (Fig. 1087) is rounded and broad behind the right lobe, but narrow on the left. Over a large part of its extent it is not covered by peritoneum; this uncovered portion is about 7.5 cm. broad at its widest part, and is in direct contact with the diaphragm. It is marked off from the upper surface by the line of reflection of the upper layer of the coronary ligament, and from the under surface by the line of reflection of the lower layer of the coronary ligament. The central part of the posterior surface presents a deep concavity which is moulded on the vertebral column and crura of the diaphragm. To the right of this the inferior vena cava is lodged in its fossa between the uncovered area and the caudate lobe. Close to the right of this fossa and immediately above the renal impression is a small triangular depressed area, the suprarenal impression, the greater part of which is devoid of peritoneum; it lodges the right suprarenal gland. To the left of the inferior vena cava is the caudate lobe, which lies between the fossa for the vena cava and the fossa for the ductus venosus. Its lower end projects and forms part of the posterior boundary of the porta; on the right, it is connected with the under surface of the right lobe of the liver by theee caudate process, and on the left it presents an elevation, the papillary process. Its posterior surface rests upon the diaphragm, being separated from it merely by the upper part of the omental bursa. To the left of the fossa for the ductus venosus is a groove in which lies the antrum cardiacum of the esophagus. | 6 |
| The anterior border (margo anterior) is thin and sharp, and marked opposite the attachment of the falciform ligament by a deep notch, the umbilical notch, and opposite the cartilage of the ninth rib by a second notch for the fundus of the gall-bladder. In adult males this border generally corresponds with the lower margin of the thorax in the right mammillary line; but in women and children it usually projects below the ribs. | 7 |
| The left extremity of the liver is thin and flattened from above downward. | 8 |
| |
| Fossæ.—The left sagittal fossa (fossa sagittalis sinistra; longitudinal fissure) is a deep groove, which extends from the notch on the anterior margin of the liver to the upper border of the posterior surface of the organ; it separates the right and left lobes. The porta joins it, at right angles, and divides it into two parts. The anterior part, or fossa for the umbilical vein, lodges the umbilical vein in the fetus, and its remains (the ligamentum teres) in the adult; it lies between the quadrate lobe and the left lobe of the liver, and is often partially bridged over by a prolongation of the hepatic substance, the pons hepatis. The posterior part, or fossa for the ductus venosus, lies between the left lobe and the caudate lobe; it lodges in the fetus, the ductus venosus, and in the adult a slender fibrous cord, the ligamentum venosum, the obliterated remains of that vessel. | 9 |
| The porta or transverse fissure (porta hepatis) is a short but deep fissure, about 5 cm. long, extending transversely across the under surface of the left portion of the right lobe, nearer its posterior surface than its anterior border. It joins nearly at right angles with the left sagittal fossa, and separates the quadrate lobe in front from the caudate lobe and process behind. It transmits the portal vein, the hepatic artery and nerves, and the hepatic duct and lymphatics. The hepatic duct lies in front and to the right, the hepatic artery to the left, and the portal vein behind and between the duct and artery. | 10 |
| The fossa for the gall-bladder (fossa vesicæ felleæ) is a shallow, oblong fossa, placed on the under surface of the right lobe, parallel with the left sagittal fossa. It extends from the anterior free margin of the liver, which is notched by it, to the right extremity of the porta. | 11 |
| The fossa for the inferior vena cava (fossa venæ cavæ) is a short deep depression, occasionally a complete canal in consequence of the substance of the liver surrounding the vena cava. It extends obliquely upward on the posterior surface between the caudate lobe and the bare area of the liver, and is separated from the porta by the caudate process. On slitting open the inferior vena cava the orifices of the hepatic veins will be seen opening into this vessel at its upper part, after perforating the floor of this fossa. | 12 |
| |
| Lobes.—The right lobe (lobus hepatis dexter) is much larger than the left; the proportion between them being as six to one. It occupies the right hypochondrium, and is separated from the left lobe on its upper surface by the falciform ligament; on its under and posterior surfaces by the left sagittal fossa; and in front by the umbilical notch. It is of a somewhat quadrilateral form, its under and posterior surfaces being marked by three fossæ: the porta and the fossæ for the gall-bladder and inferior vena cava, which separate its left part into two smaller lobes; the quadrate and caudate lobes. The impressions on the right lobe have already been described. | 13 |
| The quadrate lobe (lobus quadratus) is situated on the under surface of the right lobe, bounded in front by the anterior margin of the liver; behind by the porta; on the right, by the fossa for the gall-bladder; and on the left, by the fossa for the umbilical vein. It is oblong in shape, its antero-posterior diameter being greater than its transverse. | 14 |
| The caudate lobe (lobus caudatus; Spigelian lobe) is situated upon the posterior surface of the right lobe of the liver, opposite the tenth and eleventh thoracic vertebræ. It is bounded, below, by the porta; on the right, by the fossa for the inferior vena cava; and, on the left, by the fossa for the ductus venosus. It looks backward, being nearly vertical in position; it is longer from above downward than from side to side, and is somewhat concave in the transverse direction. The caudate process is a small elevation of the hepatic substance extending obliquely lateralward, from the lower extremity of the caudate lobe to the under surface of the right lobe. It is situated behind the porta, and separates the fossa for the gall-bladder from the commencement of the fossa for the inferior vena cava. | 15 |
| The left lobe (lobus hepatis sinister) is smaller and more flattened than the right. It is situated in the epigastric and left hypochondriac regions. Its upper surface is slightly convex and is moulded on to the diaphragm; its under surface presents the gastric impression and omental tuberosity, already referred to page 1189. | 16 |
| |
| Ligaments.—The liver is connected to the under surface of the diaphragm and to the anterior wall of the abdomen by five ligaments; four of these—the falciform, the coronary, and the two lateral—are peritoneal folds; the fifth, the round ligament, is a fibrous cord, the obliterated umbilical vein. The liver is also attached to the lesser curvature of the stomach by the hepatogastric and to the duodenum by the hepatoduodenal ligament (see page 1157). | 17 |
| The falciform ligament (ligamentum falciforme hepatis) is a broad and thin antero-posterior peritoneal fold, falciform in shape, its base being directed downward and backward, its apex upward and backward. It is situated in an antero-posterior plane, but lies obliquely so that one surface faces forward and is in contact with the peritoneum behind the right Rectus and the diaphragm, while the other is directed backward and is in contact with the left lobe of the liver. It is attached by its left margin to the under surface of the diaphragm, and the posterior surface of the sheath of the right Rectus as low down as the umbilicus; by its right margin it extends from the notch on the anterior margin of the liver, as far back as the posterior surface. It is composed of two layers of peritoneum closely united together. Its base or free edge contains between its layers the round ligament and the parumbilical veins. | 18 |
| The coronary ligament (ligamentum coronarium hepatis) consists of an upper and a lower layer. The upper layer is formed by the reflection of the peritoneum from the upper margin of the bare area of the liver to the under surface of the diaphragm, and is continuous with the right layer of the falciform ligament. The lower layer is reflected from the lower margin of the bare area on to the right kidney and suprarenal gland, and is termed the hepatorenal ligament. | 19 |
| The triangular ligaments (lateral ligaments) are two in number, right and left. The right triangular ligament (ligamentum triangulare dextrum) is situated at the right extremity of the bare area, and is a small fold which passes to the diaphragm, being formed by the apposition of the upper and lower layers of the coronary ligament. The left triangular ligament (ligamentum triangulare sinistrum) is a fold of some considerable size, which connects the posterior part of the upper surface of the left lobe to the diaphragm; its anterior layer is continuous with the left layer of the falciform ligament. | 20 |
| The round ligament (ligamentum teres hepatis) is a fibrous cord resulting from the obliteration of the umbilical vein. It ascends from the umbilicus, in the free margin of the falciform ligament, to the umbilical notch of the liver, from which it may be traced in its proper fossa on the inferior surface of the liver to the porta, where it becomes continuous with the ligamentum venosum. | 21 |
| |
| Fixation of the Liver.—Several factors contribute to maintain the liver in place. The attachments of the liver to the diaphragm by the coronary and triangular ligaments and the intervening connective tissue of the uncovered area, together with the intimate connection of the inferior vena cava by the connective tissue and hepatic veins would hold up the posterior part of the liver. Some support is derived from the pressure of the abdominal viscera which completely fill the abdomen whose muscular walls are always in a state of tonic contraction. The superior surface of the liver is perfectly fitted to the under surface of the diaphragm so that atmospheric pressure alone would be enough to hold it against the diaphragm. The latter in turn is held up by the negative pressure in the thorax. The lax falciform ligament certainly gives no support though it probably limits lateral displacement. | 22 |
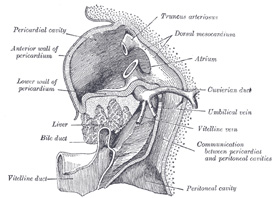 |
FIG. 1088– Liver with the septum transversum. Human embryo 3 mm. long. (After model and figure by His.) (See enlarged image) |
| |
| |
| Development.—The liver arises in the form of a diverticulum or hollow outgrowth from the ventral surface of that portion of the gut which afterward becomes the descending part of the duodenum (Fig. 1088). This diverticulum is lined by entoderm, and grows upward and forward into the septum transversum, a mass of mesoderm between the vitelline duct and the pericardial cavity, and there gives off two solid buds of cells which represent the right and the left lobes of the liver. The solid buds of cells grow into columns or cylinders, termed the hepatic cylinders, which branch and anastomose to form a close meshwork. This network invades the vitelline and umbilical veins, and breaks up these vessels into a series of capillary-like vessels termed sinusoids (Minot), which ramify in the meshes of the cellular network and ultimately form the venous capillaries of the liver. By the continued growth and ramification of the hepatic cylinders the mass of the liver is gradually formed. The original diverticulum from the duodenum forms the common bileduct, and from this the cystic duct and gall-bladder arise as a solid outgrowth which later acquires a lumen. The opening of the common duct is at first in the ventral wall of the duodenum; later, owing to the rotation of the gut, the opening is carried to the left and then dorsalward to the position it occupies in the adult. | 23 |
| As the liver undergoes enlargement, both it and the ventral mesogastrium of the fore-gut are gradually differentiated from the septum transversum; and from the under surface of the latter the liver projects downward into the abdominal cavity. By the growth of the liver the ventral mesogastrium is divided into two parts, of which the anterior forms the falciform and coronary ligaments, and the posterior the lesser omentum. About the third month the liver almost fills the abdominal cavity, and its left lobe is nearly as large as its right. From this period the relative development of the liver is less active, more especially that of the left lobe, which actually undergoes some degeneration and becomes smaller than the right; but up to the end of fetal life the liver remains relatively larger than in the adult. | 24 |
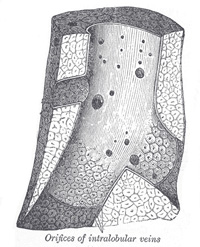 |
FIG. 1089– Longitudinal section of a hepatic vein. (After Kiernan.) (See enlarged image) |
| |
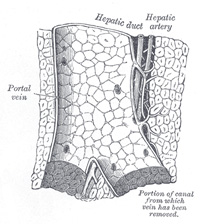 |
FIG. 1090– Longitudinal section of a small portal vein and canal. (After Kiernan.) (See enlarged image) |
| |
| |
| Vessels and Nerves.—The vessels connected with the liver are: the hepatic artery, the portal vein, and the hepatic veins. | 25 |
| The hepatic artery and portal vein, accompanied by numerous nerves, ascend to the porta, between the layers of the lesser omentum. The bile duct and the lymphatic vessels descend from the porta between the layers of the same omentum. The relative positions of the three structures are as follows: the bile duct lies to the right, the hepatic artery to the left, and the portal vein behind and between the other two. They are enveloped in a loose areolar tissue, the fibrous capsule of Glisson, which accompanies the vessels in their course through the portal canals in the interior of the organ (Fig. 1090). | 26 |
| The hepatic veins (Fig. 1089) convey the blood from the liver, and are described on page 680. They have very little cellular investment, and what there is binds their parietes closely to the walls of the canals through which they run; so that, on section of the organ, they remain widely open and are solitary, and may be easily distinguished from the branches of the portal vein, which are more or less collapsed, and always accompanied by an artery and duct. | 27 |
| The lymphatic vessels of the liver are described on page 711. | 28 |
| The nerves of the liver, derived from the left vagus and sympathetic, enter at the porta and accompany the vessels and ducts to the interlobular spaces. Here, according to Korolkow, the medullated fibers are distributed almost exclusively to the coats of the bloodvessels; while the non-medullated enter the lobules and ramify between the cells and even within them. 173 | 29 |
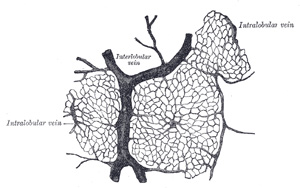 |
FIG. 1091– Section of injected liver (dog). (See enlarged image) |
| |
| |
| Structure of the Liver.—The substance of the liver is composed of lobules, held together by an extremely fine areolar tissue, in which ramify the portal vein, hepatic ducts, hepatic artery, hepatic veins, lymphatics, and nerves; the whole being invested by a serous and a fibrous coat. | 30 |
| The serous coat (tunica serosa) is derived from the peritoneum, and invests the greater part of the surface of the organ. It is intimately adherent to the fibrous coat. | 31 |
| The fibrous coat (capsula fibrosa [Glissoni]; areolar coat) lies beneath the serous investment, and covers the entire surface of the organ. It is difficult of demonstration, excepting where the serous coat is deficient. At the porta it is continuous with the fibrous capsule of Glisson, and on the surface of the organ with the areolar tissue separating the lobules. | 32 |
| The lobules (lobuli hepatis) form the chief mass of the hepatic substance; they may be seen either on the surface of the organ, or by making a section through the gland, as small granular bodies, about the size of a millet-seed, measuring from 1 to 2.5 mm. in diameter. In the human subject their outlines are very irregular; but in some of the lower animals (for example, the pig) they are well-defined, and, when divided transversely, have polygonal outlines. The bases of the lobules are clustered around the smallest radicles (sublobular) of the hepatic veins, to which each is connected (Fig. 1089) by means of a small branch which issues from the center of the lobule (intralobular). The remaining part of the surface of each lobule is imperfectly isolated from the surrounding lobules by a thin stratum of areolar tissue, in which is contained a plexus of vessels, the interlobular plexus, and ducts. In some animals, as the pig, the lobules are completely isolated from one another by the interlobular areolar tissue (Fig. 1092). | 33 |
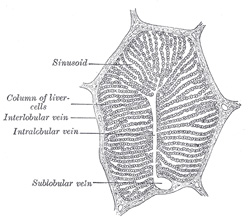 |
FIG. 1092– A single lobule of the liver of a pig. X 60. (See enlarged image) |
| |
| If one of the sublobular veins be laid open, the bases of the lobules may be seen through the thin wall of the vein on which they rest, arranged in a form resembling a tesselated pavement, the center of each polygonal space presenting a minute aperture, the mouth of an intralobular vein (Fig. 1089). | 34 |
| Microscopic Appearance (Fig. 1092).—Each lobule consists of a mass of cells, hepatic cells, arranged in irregular radiating columns between which are the blood channels (sinusoids). These convey the blood from the circumference to the center of the lobule, and end in the intralobular vein, which runs through its center, to open at its base into one of the sublobular veins. Between the cells are also the minute bile capillaries. Therefore, in the lobule there are all the essentials of a secreting gland; that is to say: (1) cells, by which the secretion is formed; (2) bloodvessels, in close relation with the cells, containing the blood from which the secretion is derived; (3) ducts, by which the secretion, when formed, is carried away. | 35 |
| 1. The hepatic cells are polyhedral in form. They vary in size from 12 to 25μ in diameter. They contain one or sometimes two distinct nuclei. The nucleus exhibits an intranuclear network and one or two refractile nucleoli. The cells usually contain granules; some of which are protoplasmic, while others consist of glycogen, fat, or an iron compound. In the lower vertebrates, e.g., frog, the cells are arranged in tubes with the bile duct forming the lumen and bloodvessels externally. According to Delépine, evidences of this arrangement can be found in the human liver. | 36 |
| 2. The Bloodvessels.—The blood in the capillary plexus around the liver cells is brought to the liver principally by the portal vein, but also to a certain extent by the hepatic artery. | 37 |
| The hepatic artery, entering the liver at the porta with the portal vein and hepatic duct, ramifies with these vessels through the portal canals. It gives off vaginal branches, which ramify in the fibrous capsule of Glisson, and appear to be destined chiefly for the nutrition of the coats of the vessels and ducts. It also gives off capsular branches, which reach the surface of the organ, ending in its fibrous coat in stellate plexuses. Finally, it gives off interlobular branches, which form a plexus outside each lobule, to supply the walls of the interlobular veins and the accompanying bile ducts. From this plexus lobular branches enter the lobule and end in the net-work of sinusoids between the cells. | 38 |
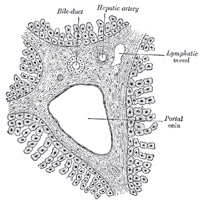 |
FIG. 1093– Section across portal canal of pig. X 250. (See enlarged image) |
| |
 |
FIG. 1094– Bile capillaries of rabbit. shown by Golgi’s method. X 450. (See enlarged image) |
| |
| The portal vein also enters at the porta, and runs through the portal canals (Fig. 1093), enclosed in Glisson’s capsule, dividing in its course into branches, which finally break up into a plexus, the interlobular plexus, in the interlobular spaces. These branches receive the vaginal and capsular veins, corresponding to the vaginal and capsular branches of the hepatic artery. Thus it will be seen that all the blood carried to the liver by the portal vein and hepatic artery finds its way into the interlobular plexus. From this plexus the blood is carried into the lobule by fine branches which converge from the circumference to the center of the lobule, and are connected by transverse branches (Fig. 1091). The walls of these small vessels are incomplete so that the blood is brought into direct relationship with the liver cells. The lining endothelium consists of irregularly branched, disconnected cells (stellate cells of Kupffer). Moreover, according to Herring and Simpson, minute channels penetrate the liver cells themselves, conveying the constituents of the blood into their substance. It will be seen that the blood capillaries of the liver lobule differ structurally from capillaries elsewhere. Developmentally they are formed by the growth of the columns of liver cells into large blood spaces or sinuses, and hence they have received the name of “sinusoids.” Arrived at the center of the lobule, the sinusoids empty themselves into one vein, of considerable size, which runs down the center of the lobule from apex to base, and is called the intralobular vein. At the base of the lobule this vein opens directly into the sublobular vein, with which the lobule is connected. The sublobular veins unite to form larger and larger trunks, and end at last in the hepatic veins, these converge to form three large trunks which open into the inferior vena cava while that vessel is situated in its fossa on the posterior surface of the liver. | 39 |
| 3. The bile ducts commence by little passages in the liver cells which communicate with canaliculi termed intercellular biliary passages (bile capillaries). These passages are merely little channels or spaces left between the contiguous surfaces of two cells, or in the angle where three or more liver cells meet (Fig. 1094), and they are always separated from the blood capillaries by at least half the width of a liver cell. The channels thus formed radiate to the circumference of the lobule, and open into the interlobular bile ducts which run in Glisson’s capsule, accompanying the portal vein and hepatic artery (Fig. 1093). These join with other ducts to form two main trunks, which leave the liver at the transverse fissure, and by their union form the hepatic duct. | 40 |
| Structure of the Ducts.—The walls of the biliary ducts consist of a connective-tissue coat, in which are muscle cells, arranged both circularly and longitudinally, and an epithelial layer, consisting of short columnar cells resting on a distinct basement membrane. | 41 |
| |
| Excretory Apparatus of the Liver.—The excretory apparatus of the liver consists of (1) the hepatic duct, formed by the junction of the two main ducts, which pass out of the liver at the porta; (2) the gall-bladder, which serves as a reservoir for the bile; (3) the cystic duct, or the duct of the gall-bladder; and (4) the common bile duct, formed by the junction of the hepatic and cystic ducts. | 42 |
| |
| The Hepatic Duct (ductus hepaticus).—Two main trunks of nearly equal size issue from the liver at the porta, one from the right, the other from the left lobe; these unite to form the hepatic duct, which passes downward and to the right for about 4 cm., between the layers of the lesser omentum, where it is joined at an acute angle by the cystic duct, and so forms the common bile duct. The hepatic duct is accompanied by the hepatic artery and portal vein. | 43 |
| The Gall-bladder (vesica fellea) (Fig. 1095).—The gall-bladder is a conical or pear-shaped musculomembranous sac, lodged in a fossa on the under surface of the right lobe of the liver, and extending from near the right extremity of the porta to the anterior border of the organ. It is from 7 to 10 cm. in length, 2.5 cm. in breadth at its widest part, and holds from 30 to 35 c.c. It is divided into a fundus, body, and neck. The fundus, or broad extremity, is directed downward, forward, and to the right, and projects beyond the anterior border of the liver; the body and neck are directed upward and backward to the left. The upper surface of the gall-bladder is attached to the liver by connective tissue and vessels. The under surface is covered by peritoneum, which is reflected on to it from the surface of the liver. Occasionally the whole of the organ is invested by the serous membrane, and is then connected to the liver by a kind of mesentery. | 44 |
 |
FIG. 1095– The gall-bladder and bile ducts laid open. (Spalteholz.) (See enlarged image) |
| |
| |
| Relations.—The body is in relation, by its upper surface, with the liver; by its under surface, with the commencement of the transverse colon; and farther back usually with the upper end of the descending portion of the duodenum, but sometimes with the superior portion of the duodenum or pyloric end of the stomach. The fundus is completely invested by peritoneum; it is in relation, in front, with the abdominal parietes, immediately below the ninth costal cartilage; behind with the transverse colon. The neck is narrow, and curves upon itself like the letter S; at its point of connection with the cystic duct it presents a well-marked constriction. | 45 |
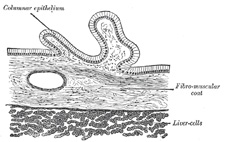 |
FIG. 1096– Transverse section of gall-bladder. (See enlarged image) |
| |
| |
| Structure (Fig. 1096).—The gall-bladder consists of three coats: serous, fibromuscular, and mucous. | 46 |
| The external or serous coat (tunica serosa vesicæ felleæ) is derived from the peritoneum; it completely invests the fundus, but covers the body and neck only on their under surfaces. | 47 |
| The fibromuscular coat (tunica muscularis vesicæ felleæ), a thin but strong layer forming the frame-work of the sac, consists of dense fibrous tissue, which interlaces in all directions, and is mixed with plain muscular fibers, disposed chiefly in a longitudinal direction, a few running transversely. | 48 |
| The internal or mucous coat (tunica mucosa vesicæ felleæ) is loosely connected with the fibrous layer. It is generally of a yellowish-brown color, and is elevated into minute rugæ. Opposite the neck of the gall-bladder the mucous membrane projects inward in the form of oblique ridges or folds, forming a sort of spiral valve. | 49 |
| The mucous membrane is continuous through the hepatic duct with the mucous membrane lining the ducts of the liver, and through the common bile duct with the mucous membrane of the duodenum. It is covered with columnar epithelium, and secretes mucin; in some animals it secretes a nucleoprotein instead of mucin. | 50 |
| The Cystic Duct (ductus cysticus).—The cystic duct about 4 cm. long, runs backward, downward, and to the left from the neck of the gall-bladder, and joins the hepatic duct to form the common bile duct. The mucous membrane lining its interior is thrown into a series of crescentic folds, from five to twelve in number, similar to those found in the neck of the gall-bladder. They project into the duct in regular succession, and are directed obliquely around the tube, presenting much the appearance of a continuous spiral valve. When the duct is distended, the spaces between the folds are dilated, so as to give to its exterior a twisted appearance. | 51 |
| The Common Bile Duct (ductus choledochus).—The common bile duct is formed by the junction of the cystic and hepatic ducts; it is about 7.5 cm. long, and of the diameter of a goose-quill. | 52 |
| It descends along the right border of the lesser omentum behind the superior portion of the duodenum, in front of the portal vein, and to the right of the hepatic artery; it then runs in a groove near the right border of the posterior surface of the head of the pancreas; here it is situated in front of the inferior vena cava, and is occasionally completely imbedded in the pancreatic substance. At its termination it lies for a short distance along the right side of the terminal part of the pancreatic duct and passes with it obliquely between the mucous and muscular coats. The two ducts unite and open by a common orifice upon the summit of the duodenal papilla, situated at the medial side of the descending portion of the duodenum, a little below its middle and about 7 to 10 cm. from the pylorus (Fig. 1100). The short tube formed by the union of the two ducts is dilated into an ampulla, the ampulla of Vater. | 53 |
| |
| Structure.—The coats of the large biliary ducts are an external or fibrous, and an internal or mucous. The fibrous coat is composed of strong fibroareolar tissue, with a certain amount of muscular tissue, arranged, for the most part, in a circular manner around the duct. The mucous coat is continuous with the lining membrane of the hepatic ducts and gall-bladder, and also with that of the duodenum; and, like the mucous membrane of these structures, its epithelium is of the columnar variety. It is provided with numerous mucous glands, which are lobulated and open by minute orifices scattered irregularly in the larger ducts. | 54 |