| The pancreas (Figs. 1097, 1098) is a compound racemose gland, analogous in its structures to the salivary glands, though softer and less compactly arranged than those organs. Its secretion, the pancreatic juice, carried by the pancreatic duct to the duodenum, is an important digestive fluid. In addition the pancreas has an important internal secretion, probably elaborated by the cells of Langerhans, which is taken up by the blood stream and is concerned with sugar metabolism. It is long and irregularly prismatic in shape; its right extremity, being broad, is called the head, and is connected to the main portion of the organ, or body, by a slight constriction, the neck; while its left extremity gradually tapers to form the tail. It is situated transversely across the posterior wall of the abdomen, at the back of the epigastric and left hypochondriac regions. Its length varies from 12.5 to 15 cm., and its weight from 60 to 100 gm. | 1 |
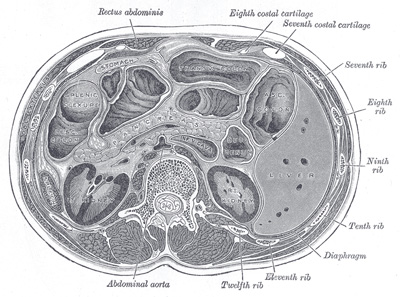 |
FIG. 1097– Transverse section through the middle of the first lumbar vertebra, showing the relations of the pancreas. (Braune.) (See enlarged image) |
| |
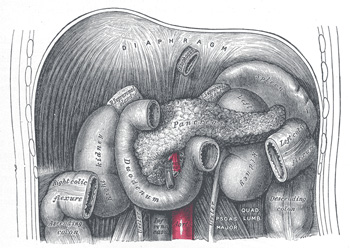 |
FIG. 1098– The duodenum and pancreas. (See enlarged image) |
| |
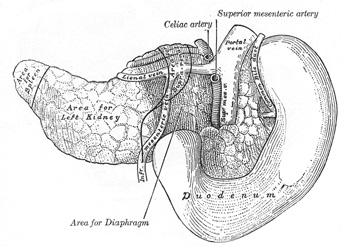 |
FIG. 1099– The pancreas and duodenum from behind. (From model by His.) (See enlarged image) |
| |
| |
| Relations.—The Head (caput pancreatis) is flattened from before backward, and is lodged within the curve of the duodenum. Its upper border is overlapped by the superior part of the duodenum and its lower overlaps the horizontal part; its right and left borders overlap in front, and insinuate themselves behind, the descending and ascending parts of the duodenum respectively. The angle of junction of the lower and left lateral borders forms a prolongation, termed the uncinate process. In the groove between the duodenum and the right lateral and lower borders in front are the anastomosing superior and inferior pancreaticoduodenal arteries; the common bile duct descends behind, close to the right border, to its termination in the descending part of the duodenum. | 2 |
| |
| Anterior Surface.—The greater part of the right half of this surface is in contact with the transverse colon, only areolar tissue intervening. From its upper part the neck springs, its right limit being marked by a groove for the gastroduodenal artery. The lower part of the right half, below the transverse colon, is covered by peritoneum continuous with the inferior layer of the transverse mesocolon, and is in contact with the coils of the small intestine. The superior mesenteric artery passes down in front of the left half across the uncinate process; the superior mesenteric vein runs upward on the right side of the artery and, behind the neck, joins with the lienal vein to form the portal vein. | 3 |
| |
| Posterior Surface.—The posterior surface is in relation with the inferior vena cava, the common bile duct, the renal veins, the right crus of the diaphragm, and the aorta. | 4 |
| The Neck springs from the right upper portion of the front of the head. It is about 2.5 cm. long, and is directed at first upward and forward, and then upward and to the left to join the body; it is somewhat flattened from above downward and backward. Its antero-superior surface supports the pylorus; its postero-inferior surface is in relation with the commencement of the portal vein; on the right it is grooved by the gastroduodenal artery. | 5 |
| The Body (corpus pancreatis) is somewhat prismatic in shape, and has three surfaces: anterior, posterior, and inferior. | 6 |
| The anterior surface (facies anterior) is somewhat concave; and is directed forward and upward: it is covered by the postero-inferior surface of the stomach which rests upon it, the two organs being separated by the omental bursa. Where it joins the neck there is a well-marked prominence, the tuber omentale, which abuts against the posterior surface of the lesser omentum. | 7 |
| The posterior surface (facies posterior) is devoid of peritoneum, and is in contact with the aorta, the lienal vein, the left kidney and its vessels, the left suprarenal gland, the origin of the superior mesenteric artery, and the crura of the diaphragm. | 8 |
| The inferior surface (facies inferior) is narrow on the right but broader on the left, and is covered by peritoneum; it lies upon the duodenojejunal flexure and on some coils of the jejunum; its left extremity rests on the left colic flexure. | 9 |
| The superior border (margo superior) is blunt and flat to the right; narrow and sharp to the left, near the tail. It commences on the right in the omental tuberosity, and is in relation with the celiac artery, from which the hepatic artery courses to the right just above the gland, while the lienal artery runs toward the left in a groove along this border. | 10 |
| The anterior border (margo anterior) separates the anterior from the inferior surface, and along this border the two layers of the transverse mesocolon diverge from one another; one passing upward over the anterior surface, the other backward over the inferior surface. | 11 |
| The inferior border (margo inferior) separates the posterior from the inferior surface; the superior mesenteric vessels emerge under its right extremity. | 12 |
| The Tail (cauda pancreatis) is narrow; it extends to the left as far as the lower part of the gastric surface of the spleen, lying in the phrenicolienal ligament, and it is in contact with the left colic flexure. | 13 |
| Birmingham described the body of the pancreas as projecting forward as a prominent ridge into the abdominal cavity and forming part of a shelf on which the stomach lies. “The portion of the pancreas to the left of the middle line has a very considerable antero-posterior thickness; as a result the anterior surface is of considerable extent; it looks strongly upward, and forms a large and important part of the shelf. As the pancreas extends to the left toward the spleen it crosses the upper part of the kidney, and is so moulded on to it that the top of the kidney forms an extension inward and backward of the upper surface of the pancreas and extends the bed in this direction. On the other hand, the extremity of the pancreas comes in contact with the spleen in such a way that the plane of its upper surface runs with little interruption upward and backward into the concave gastric surface of the spleen, which completes the bed behind and to the left, and, running upward, forms a partial cap for the wide end of the stomach. 174 | 14 |
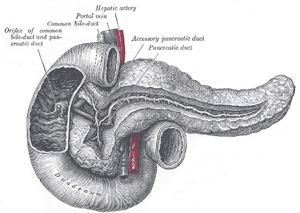 |
FIG. 1100– The pancreatic duct. (See enlarged image) |
| |
| The Pancreatic Duct (ductus pancreaticus [Wirsungi]; duct of Wirsung) extends transversely from left to right through the substance of the pancreas (Fig. 1100). It commences by the junction of the small ducts of the lobules situated in the tail of the pancreas, and, running from left to right through the body, it receives the ducts of the various lobules composing the gland. Considerably augmented in size, it reaches the neck, and turning downward, backward, and to the right, it comes into relation with the common bile duct, which lies to its right side; leaving the head of the gland, it passes very obliquely through the mucous and muscular coats of the duodenum, and ends by an orifice common to it and the common bile duct upon the summit of the duodenal papilla, situated at the medial side of the descending portion of the duodenum, 7.5 to 10 cm. below the pylorus. The pancreatic duct, near the duodenum, is about the size of an ordinary quill. Sometimes the pancreatic duct and the common bile duct open separately into the duodenum. Frequently there is an additional duct, which is given off from the pancreatic duct in the neck of the pancreas and opens into the duodenum about 2.5 cm. above the duodenal papilla. It receives the ducts from the lower part of the head, and is known as the accessory pancreatic duct (duct of Santorini). | 15 |
| |
| Development (Figs. 1101, 1102).—The pancreas is developed in two parts, a dorsal and a ventral. The former arises as a diverticulum from the dorsal aspect of the duodenum a short distance above the hepatic diverticulum, and, growing upward and backward into the dorsal mesogastrium, forms a part of the head and uncinate process and the whole of the body and tail of the pancreas. The ventral part appears in the form of a diverticulum from the primitive bile-duct and forms the remainder of the head and uncinate process of the pancreas. The duct of the dorsal part (accessory pancreatic duct) therefore opens independently into the duodenum, while that of the ventral part (pancreatic duct) opens with the common bile-duct. About the sixth week the two parts of the pancreas meet and fuse and a communication is established between their ducts. After this has occurred the terminal part of the accessory duct, i. e., the part between the duodenum and the point of meeting of the two ducts, undergoes little or no enlargement, while the pancreatic duct increases in size and forms the main duct of the gland. The opening of the accessory duct into the duodenum is sometimes obliterated, and even when it remains patent it is probable that the whole of the pancreatic secretion is conveyed through the pancreatic duct. | 16 |
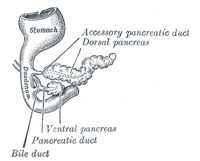 |
FIG. 1101– Pancreas of a human embryo of five weeks. (Kollmann.) (See enlarged image) |
| |
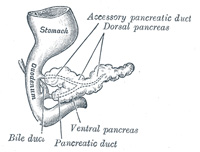 |
FIG. 1102– Pancreas of a human embryo at end of sixth week. (Kollmann.) (See enlarged image) |
| |
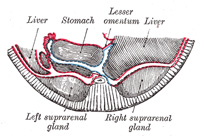 |
FIG. 1103– Schematic and enlarged cross-section through the body of a human embryo in the region of the mesogastrium. Beginning of third month. (Toldt.) (See enlarged image) |
| |
| At first the pancreas is directed upward and backward between the two layers of the dorsal mesogastrium, which give to it a complete peritoneal investment, and its surfaces look to the right and left. With the change in the position of the stomach the dorsal mesogastrium is drawn downward and to the left, and the right side of the pancreas is directed backward and the left forward (Fig. 1103). The right surface becomes applied to the posterior abdominal wall, and the peritoneum which covered it undergoes absorption (Fig. 1104); and thus, in the adult, the gland appears to lie behind the peritoneal cavity. | 17 |
| |
| Structure (Fig. 1105).—In structure, the pancreas resembles the salivary glands. It differs from them, however, in certain particulars, and is looser and softer in its texture. It is not enclosed in a distinct capsule, but is surrounded by areolar tissue, which dips into its interior, and connects together the various lobules of which it is composed. Each lobule, like the lobules of the salivary glands, consists of one of the ultimate ramifications of the main duct, ending in a number of cecal pouches or alveoli, which are tubular and somewhat convoluted. The minute ducts connected with the alveoli are narrow and lined with flattened cells. The alveoli are almost completely filled with secreting cells, so that scarcely any lumen is visible. In some animals spindle-shaped cells occupy the center of the alveolus and are known as the centroacinar cells of Langerhans. These are prolongations of the terminal ducts. The true secreting cells which line the wall of the alveolus are very characteristic. They are columnar in shape and present two zones: an outer one, clear and finely striated next the basement membrane, and an inner granular one next the lumen. In hardened specimens the outer zone stains deeply with various dyes, whereas the inner zone stains slightly. During activity the granular zone gradually diminishes in size, and when exhausted is only seen as a small area next to the lumen. During the resting stages it gradually increases until it forms nearly three-fourths of the cell. In some of the secreting cells of the pancreas is a spherical mass, staining more easily than the rest of the cell; this is termed the paranucleus, and is believed to be an extension from the nucleus. The connective tissue between the alveoli presents in certain parts collections of cells, which are termed interalveolar cell islets (islands of Langerhans). The cells of these stain lightly with hematoxylin or carmine, and are more or less polyhedral in shape, forming a net-work in which ramify many capillaries. There are two main types of cell in the islets, distinguished as A-cells and B-cells according to the special staining reactions of the granules they contain. The cell islets have been supposed to produce the internal secretion of the pancreas which is necessary for carbohydrate metabolism, but numerous researches have so far failed to elucidate their real function. | 18 |
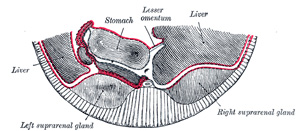 |
FIG. 1104– Section through same region as in Fig. 1103, at end of third month. (Toldt.) (See enlarged image) |
| |
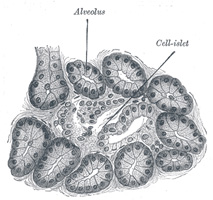 |
FIG. 1105– Section of pancreas of dog. X 250. (See enlarged image) |
| |
| The walls of the pancreatic duct are thin, consisting of two coats, an external fibrous and an internal mucous; the latter is smooth, and furnished near its termination with a few scattered follicles. | 19 |
| |
| Vessels and Nerves.—The arteries of the pancreas are derived from the lienal, and the pancreaticoduodenal branches of the hepatic and superior mesenteric. Its veins open into the lienal and superior mesenteric veins. Its lymphatics are described on page 711. Its nerves are filaments from the lienal plexus. | 20 |